Cynnwys
- Main points
- Statistician’s comment
- Things you need to know about this release
- Men’s most common age at death is 86.4 years in the UK
- Life expectancy has improved fastest in the London borough of Camden
- Gain in life expectancy at birth has slowed in the UK in recent years
- Females live three years longer in “not good” health than males in the UK
- People living in Scotland spend the highest proportion of life in “good” health, despite having the lowest life expectancy
- Healthy life expectancy at birth differs by 18 years across UK local areas
- Local area gap in years lived in good health exceeds 10 years among pensioners in the UK
- Quality and methodology
1. Main points
This bulletin presents two additional measures of longevity for the first time; namely the median and modal ages at death; these alternative measures provide additional information on longevity patterns over time.
It is estimated that half of newborns in the UK could expect to still be alive at the age of 82.3 years if male and 85.8 years if female; the largest number of deaths for males are expected to occur at age 86.4 years and at age 88.9 for females, if they experience the same mortality rates as were observed in the period 2014 to 2016.
Over the past 15 years, the most common age at death (the modal age at death) for males has increased twice as fast compared with females and faster than traditional life expectancy.
The rate of improvement in life expectancy at birth in the UK during the first half of the second decade of the 21st century was 75.3% lower for males and 82.7% lower for females when compared with the first half of the first decade; therefore, improvements in life expectancy have slowed during the second decade.
Healthy life expectancy (HLE) at birth for males was 63.1 years and for females was 63.7 years in 2014 to 2016.
Females continue to live more years in good health than males, despite their HLE decreasing by 1.7 months since 2009 to 2011 and that of males increasing by 4.3 months over the same period.
HLE at birth across local areas of the UK varies by 18 years, while disability-free life expectancy (DFLE) at birth varies by 20 years.
2. Statistician’s comment
“This analysis supports the view that mortality improvements in the UK have slowed somewhat in the second decade of the 21st century. This is evidenced by the rate of improvement in life expectancy at birth in the UK falling by 75.3% for males and 82.7% for females when comparing the first half of the second decade with the first half of the first decade.”
Chris White, Principal Research Officer, Office for National Statistics
Nôl i'r tabl cynnwys3. Things you need to know about this release
This bulletin includes content not previously included:
we report the median and modal ages at death; these measures have been calculated for the UK and constituent countries only, and exclude English regions, counties and local areas
an analysis of the change in life expectancy since 2001 to 2003 across local areas, to inform the debate on how uniform the stalling of mortality improvement observed in national analyses has been across local areas of the UK
estimates of healthy life expectancy (HLE) and disability-free life expectancy (DFLE) are included for some metropolitan counties, including Greater Manchester and the West Midlands, for the first time
dynamic interactive maps are available for tracking an area’s life expectancy over time and how it compares with national estimates
The life expectancy estimates reported in this release are period-based life expectancies. This is a measure of the average number of years a person would live from a given age, if he or she experienced the particular area’s age-specific mortality rates for that time period throughout his or her life. This measure makes no allowance for any future actual or projected changes in mortality. In practice, a population’s death rates are likely to change in the future, so period-based life expectancy does not therefore give the number of years someone would actually expect to live. Also, people may live in other areas for at least some part of their lives.
Healthy life expectancy (HLE) is an estimate of the number of years lived in “Very good” or “Good” general health, based on how individuals perceive their general health. Disability-free life expectancy (DFLE) is an estimate of the number of years lived without a long-lasting physical or mental health condition that limits daily activities.
The median age at death measures the age at which half a hypothetical cohort would still be alive; the modal age at death measures the age at which deaths most commonly occur. The median and modal age groups are identified using the expected deaths obtained from the life table, which is derived from the probability of dying in the age interval. The modal age group is where the largest number of deaths occurred, while the median age group is where the cumulative expected deaths across age groups exceed half the total expected deaths. Formulae for grouped data are then applied to obtain approximate median and modal ages at death from the abridged life table.
Separate life tables closed at age 95 and over were used to estimate the median and modal ages at death for comparison with traditional life expectancy. However, in all other instances, life expectancy was estimated using a life table closed at age 90 and over, and it is these estimates that should be used for subnational comparison.
Subnational life expectancy estimates for Scotland’s council areas and Northern Ireland’s local government districts have been calculated using the same method as for England and Wales. Responsibility for the production of other statistics for Scotland and Northern Ireland are with the National Records Scotland (NRS) and Northern Ireland Statistics and Research Agency (NISRA) respectively.
Subnational HLE and DFLE estimates for Wales, Scotland and Northern are also available:
Scottish Public Health Observatory (ScotPHO)
This release accompanies an investigation into health state prevalence estimation using alternative methods for national and subnational reporting of health state life expectancies. The findings of this investigation are published alongside this release as a separate article and we are consulting users and invite them to share their views on these proposed changes before implementation. A consultation document is available for providing feedback and this consultation opens on 7 December 2017 and will close on 8 February 2018.
Nôl i'r tabl cynnwys4. Men’s most common age at death is 86.4 years in the UK
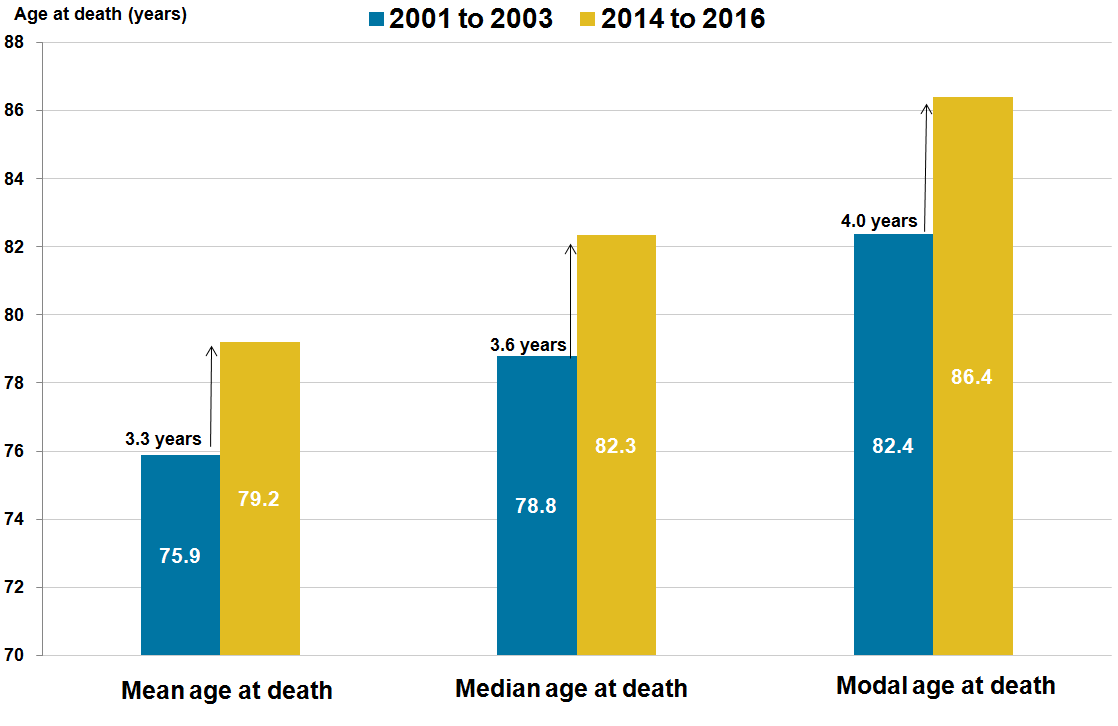
If age specific mortality rates observed in the period 2014 to 2016 continue into the future, males born in the UK in 2014 to 2016 will expect to live on average 79.2 years. However, half of this cohort will expect to still be alive at age 82.3 years (the median age at death) and this cohort’s most common age at death is expected to be 86.4 years (the modal age at death). The equivalent median and modal ages at death for females were 85.8 years and 88.9 years.
From these results, it is clear that the modal age at death exceeds the median, which itself is higher than life expectancy at birth, which is a measure of the mean age at death. This is because deaths are concentrated at older ages and both the median and modal age at death are affected more by deaths at older ages, whereas traditional life expectancy takes account of deaths across all ages and is more sensitive to premature mortality.
It is noticeable from Figure 1 that the modal age at death has improved markedly in contrast with the median and life expectancy (the mean age at death). This suggests that the extent of improvement in males’ mortality is concentrated more at older ages than females’.
Figure 1: Mean age at death (traditional life expectancy at birth), median and modal ages at death, males, UK, 2001 to 2003 and 2014 to 2016
Source: Office for National Statistics
Download this image Figure 1: Mean age at death (traditional life expectancy at birth), median and modal ages at death, males, UK, 2001 to 2003 and 2014 to 2016
.png (28.2 kB) .xls (26.1 kB)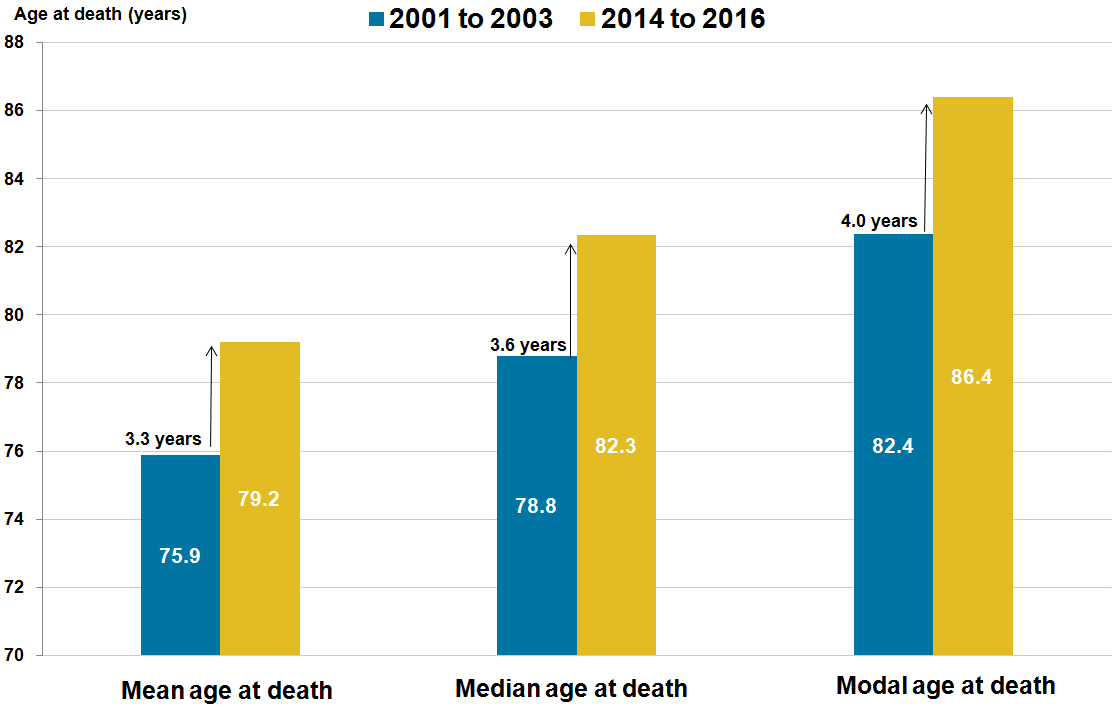{kind=link}
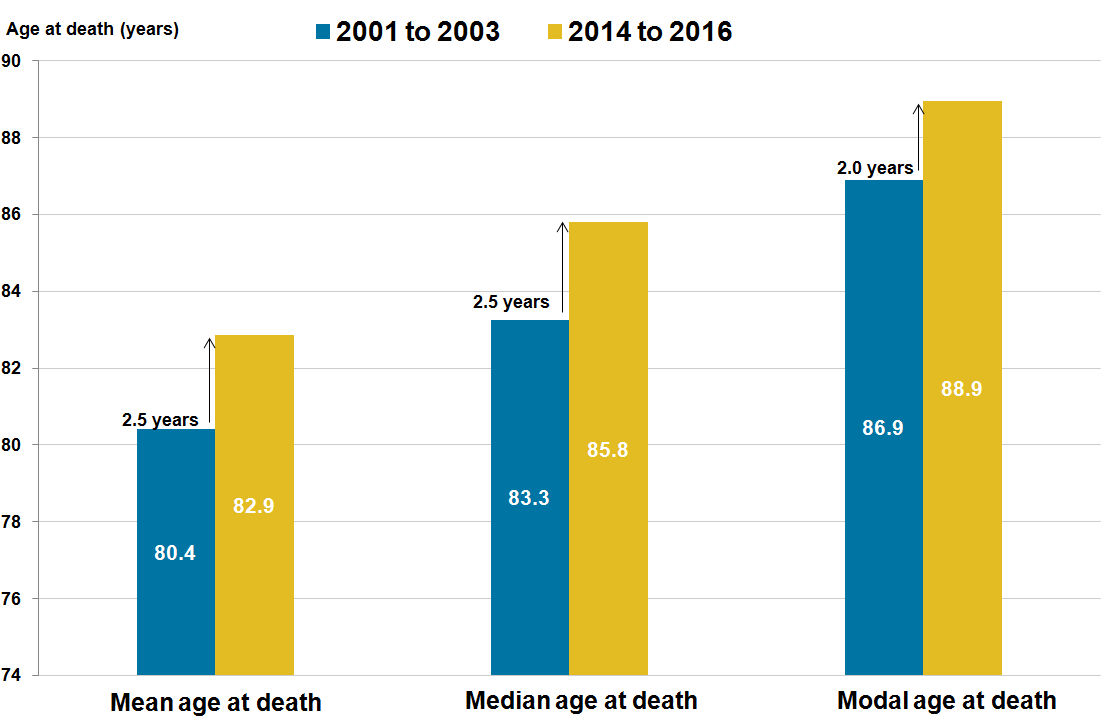
As female longevity is higher than males, their most common age at death is comparatively higher than males (Figure 2).
In 2014 to 2016, the female modal age at death was 88.9 years, which was 2.6 years higher than that of males. However, when comparing the change in the modal age at death over the past 15 years, the modal age at death for males has grown twice as quickly as females. This is further evidenced by a closing of the gap between male and female longevity observed since the early 1980s, caused by more rapid improvements in male mortality.
For females, Figure 2 also shows that the gain in life expectancy and the median age at death (2.5 years for both measures) are faster than the gain in modal age at death (2.0 years). This suggests that improvements in female mortality are less concentrated at older ages, as was the case for males.
For the constituent countries, all three measures of average life span (life expectancy, median and modal ages at death) are provided in the accompanying datasets. Life expectancy at birth based on a life table closed at age 95 and over should only be used in making comparisons with the median and modal ages at death. Life expectancy estimates reported in subsequent sections are based on a life table closed at age 90 and over and are appropriate for comparing differences between local populations, benchmarking against national estimates and for the detection of improvements over time.
Figure 2: Mean age at death (traditional life expectancy at birth), median and modal ages at death, females, UK, 2001 to 2003 and 2014 to 2016
Source: Office for National Statistics
Download this image Figure 2: Mean age at death (traditional life expectancy at birth), median and modal ages at death, females, UK, 2001 to 2003 and 2014 to 2016
.png (28.7 kB) .xls (26.1 kB)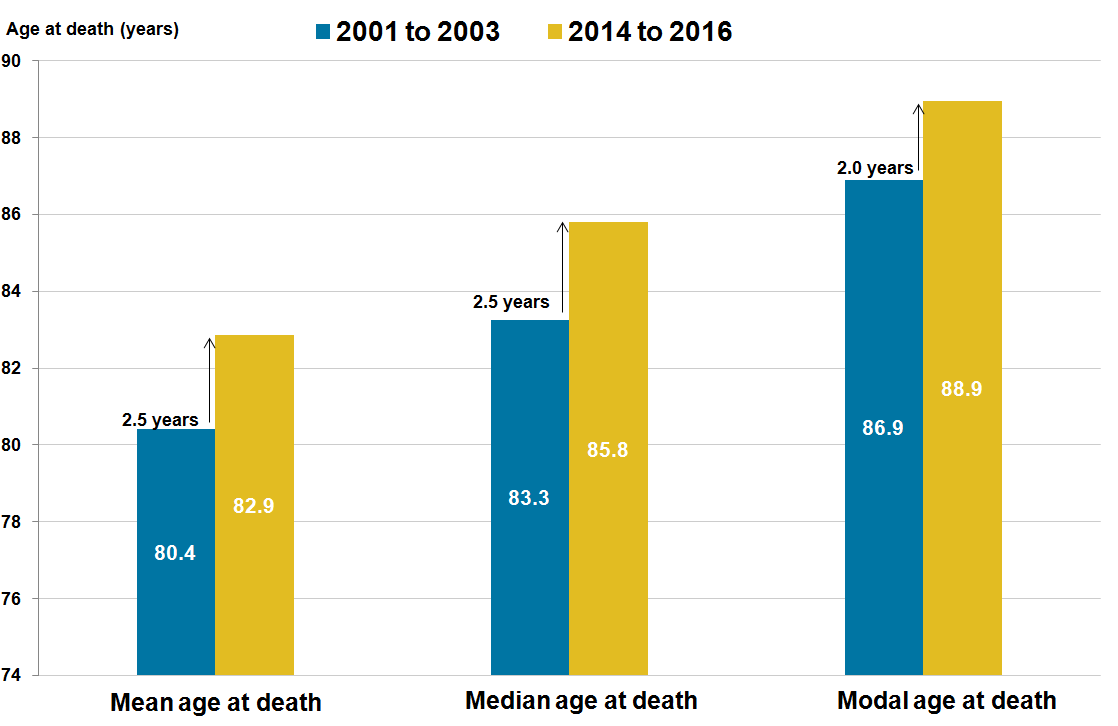{kind=link}
5. Life expectancy has improved fastest in the London borough of Camden
Across local areas in the UK between 2001 to 2003 and 2014 to 2016, the largest improvement in life expectancy at birth was observed in the London borough of Camden for males (7.5 years) and females (5.8 years). The smallest improvement was in Denbighshire for males (1.4 years) and Kingston upon Hull for females (0.7 years).
This release includes life expectancy estimates for local areas across the UK, in addition to constituent countries and English regions, from 2001 to 2003 and 2014 to 2016. These estimates are available in datasets and include confidence intervals to assist users in making judgments about the statistical significance of period-specific differences and changes over time.
To illustrate how life expectancy has changed over time, Figure 3 shows life expectancy at birth and age 65 across local areas in the UK. This provides an opportunity for local areas to compare life expectancy at these ages against the UK.
Figure 3: Life expectancy at birth and age 65 by sex across local areas in the UK, between 2001 to 2003 and 2014 to 2016
Embed code
6. Gain in life expectancy at birth has slowed in the UK in recent years
Figure 4 shows the direction of travel in life expectancy at birth using the difference between temporally distinct adjacent periods. The strongest gains for males were observed between 2007 to 2009 and 2010 to 2012. Subsequent comparative periods have witnessed sharp decreases in growth, such that the improvement observed between 2011 to 2013 and 2014 to 2016 is the smallest so far this century. The pattern is similar for females, but the magnitude of improvement is much smaller across all comparative periods.
Figure 4: Gain in life expectancy at birth in UK by sex over rolling temporally distinct periods, 2001 to 2003 and 2014 to 2016
Source: Office for National Statistics
Notes:
- To report the gain in life expectancy at birth, temporally distinct adjacent periods are subtracted. The year 2001-2006 on the x-axis reflects the gains between 2001 to 2003 and 2004 to 2006, and similarly years 2011-2016 between 2011 to 2013 and 2014 to 2016.
Download this chart Figure 4: Gain in life expectancy at birth in UK by sex over rolling temporally distinct periods, 2001 to 2003 and 2014 to 2016
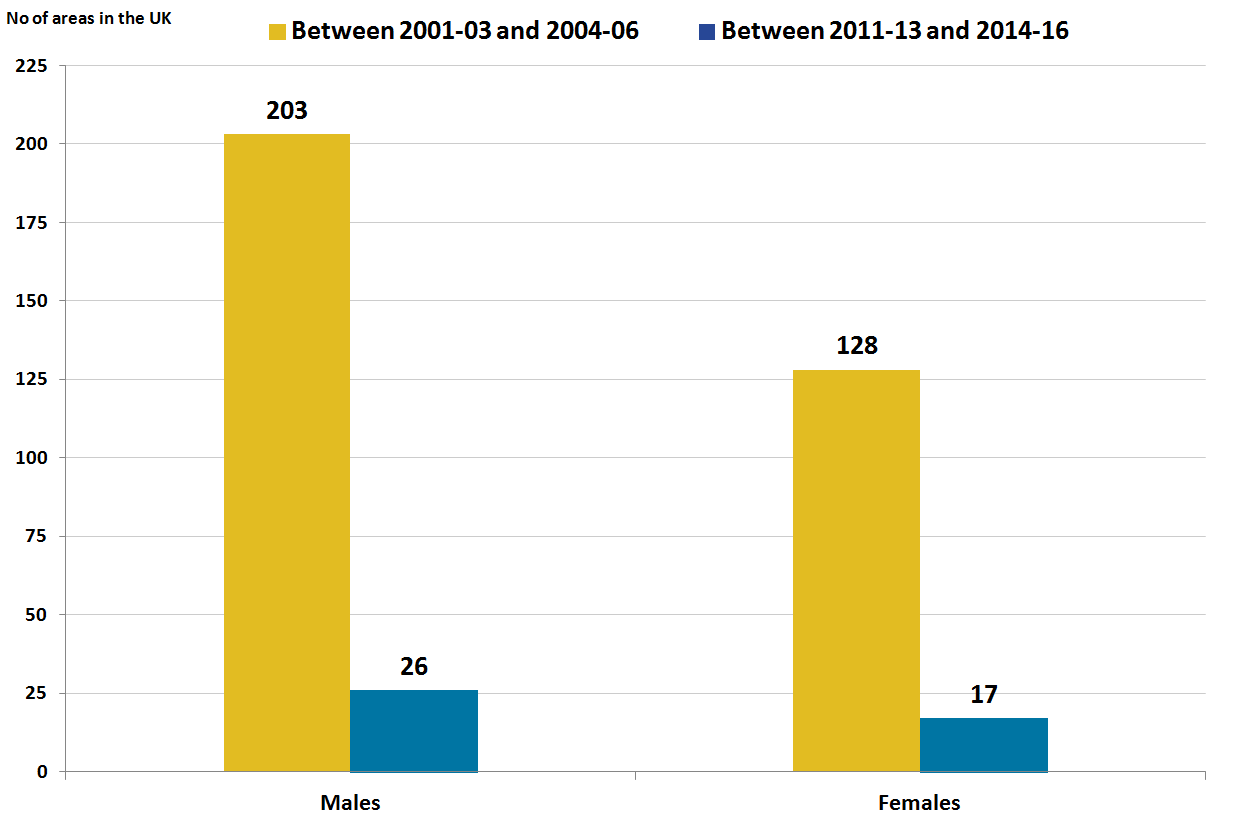
Image .csv .xlsAt subnational level, a similar pattern was mostly observed. Figure 5 shows the number of local areas across the UK where statistically significant increases in life expectancy at birth occurred over time. As shown by Figure 5, the number of local areas that achieved a statistically significant gain in life expectancy has decreased notably since the improvement that occurred between 2001 to 2003 and 2004 to 2006. This suggests that the stalling in life expectancy improvement is widespread across local areas of the UK.
Figure 5: Number of areas across UK where gain in life expectancy at birth were statistically significant, between 2001 to 2003 and 2014 to 2016
Source: Office for National Statistics
Notes:
Statistical significant was examined by one-tailed Z scores. Detailed information about this can be viewed in Appendix 1 of the Sullivan guide.
Local areas are lower tier local authorities in England, unitary authorities in Wales, council areas in Scotland and local government districts in Northern Ireland.
Excluded areas are the Isles of Scilly and City of London because of small populations.
Mid Ulster in Northern Ireland for males was the only area where a statistically significant fall in life expectancy at birth occurred between 2001 to 2003 and 2004 to 2006.
Southend-on-Sea for males and Amber Valley for females stood out as two areas out of 7 areas, where there was a statistically significant fall in life expectancy at birth between 2011 to 2013 and 2014 to 2016
Download this image Figure 5: Number of areas across UK where gain in life expectancy at birth were statistically significant, between 2001 to 2003 and 2014 to 2016
.png (21.3 kB) .xls (396.8 kB)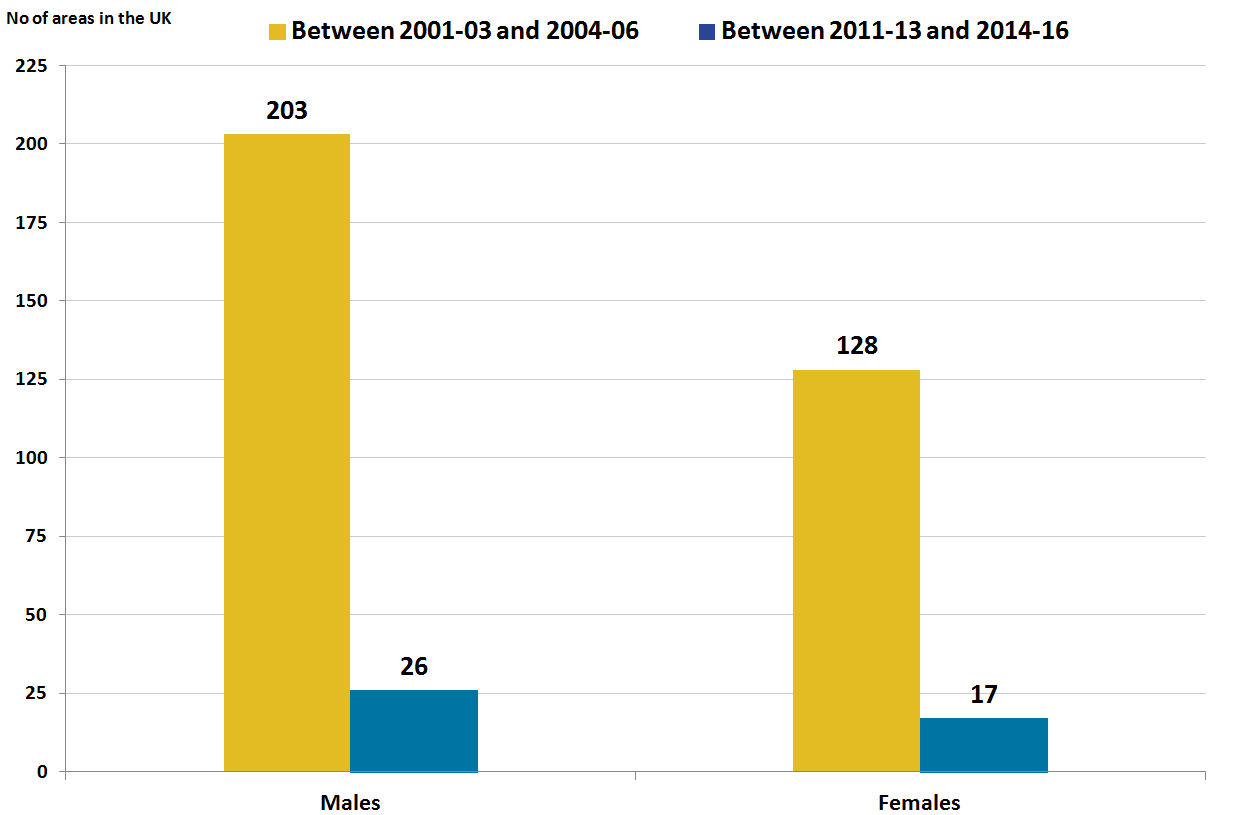{kind=link}
The change in life expectancy is illustrated in Figure 6, which shows the gain in life expectancy at birth in months across local areas in the UK. The gain is based on temporally distinct adjacent periods. When an area is selected, a negative value indicates life expectancy has fallen.
Figure 6: Gain in life expectancy at birth in months by sex across local areas in the UK, using temporally distinct adjacent periods between 2001 to 2003 and 2014 to 2016
Embed code
7. Females live three years longer in “not good” health than males in the UK
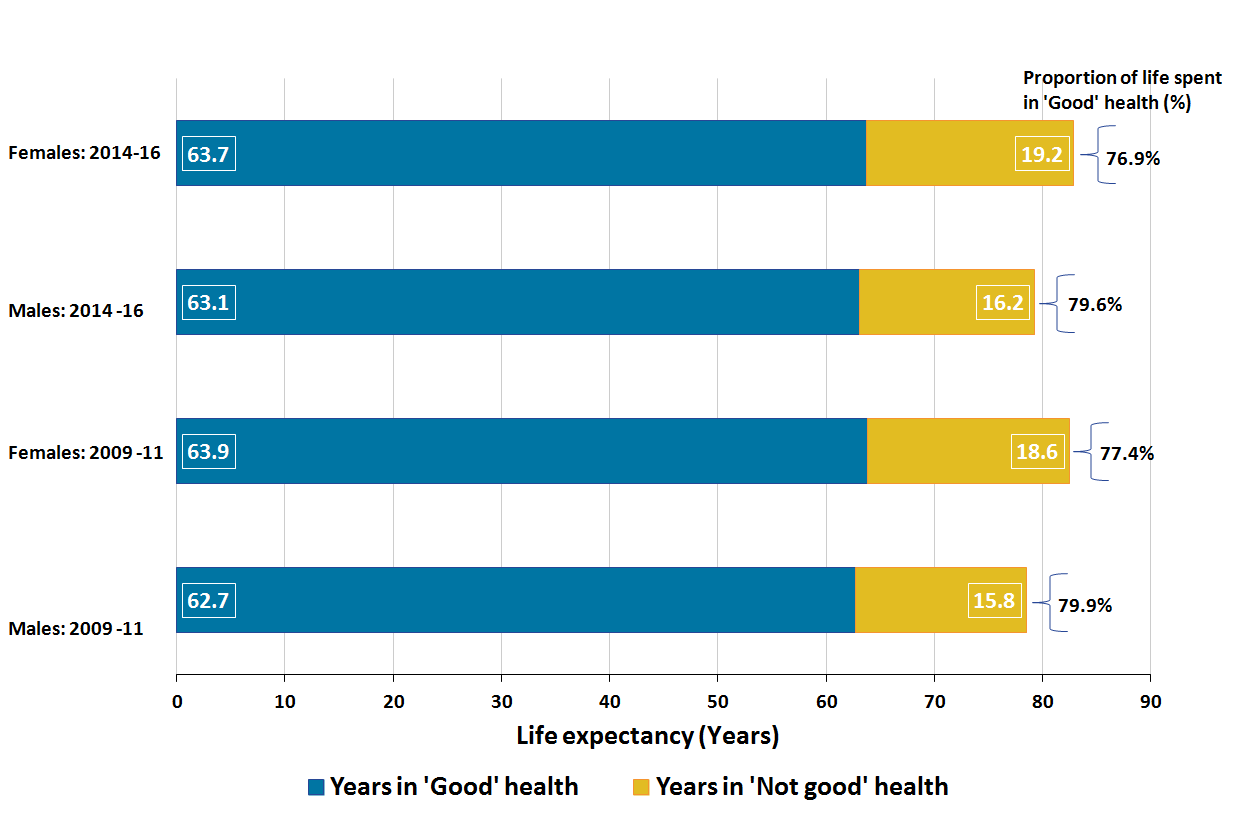
Figure 7 reports life expectancy and healthy life expectancy (HLE) at birth, together with the proportion of life spent in good health observed in the periods 2009 to 2011 and 2014 to 2016.
Figure 7: Healthy life expectancy, life expectancy and the proportion of life spent healthy at birth, by sex in the UK, 2009 to 2011 and 2014 to 2016
Source: Annual Population Survey, Office for National Statistics
Notes:
Survey respondents who answered their general health as ‘very good’ and ‘good’ were classified as having 'Good' health. Those who answered ‘fair’ ‘bad’ and ‘very bad’ were classified as having 'Not good' health.
Figures may not sum because of the rounding.
Download this image Figure 7: Healthy life expectancy, life expectancy and the proportion of life spent healthy at birth, by sex in the UK, 2009 to 2011 and 2014 to 2016
.png (33.5 kB) .xls (27.1 kB)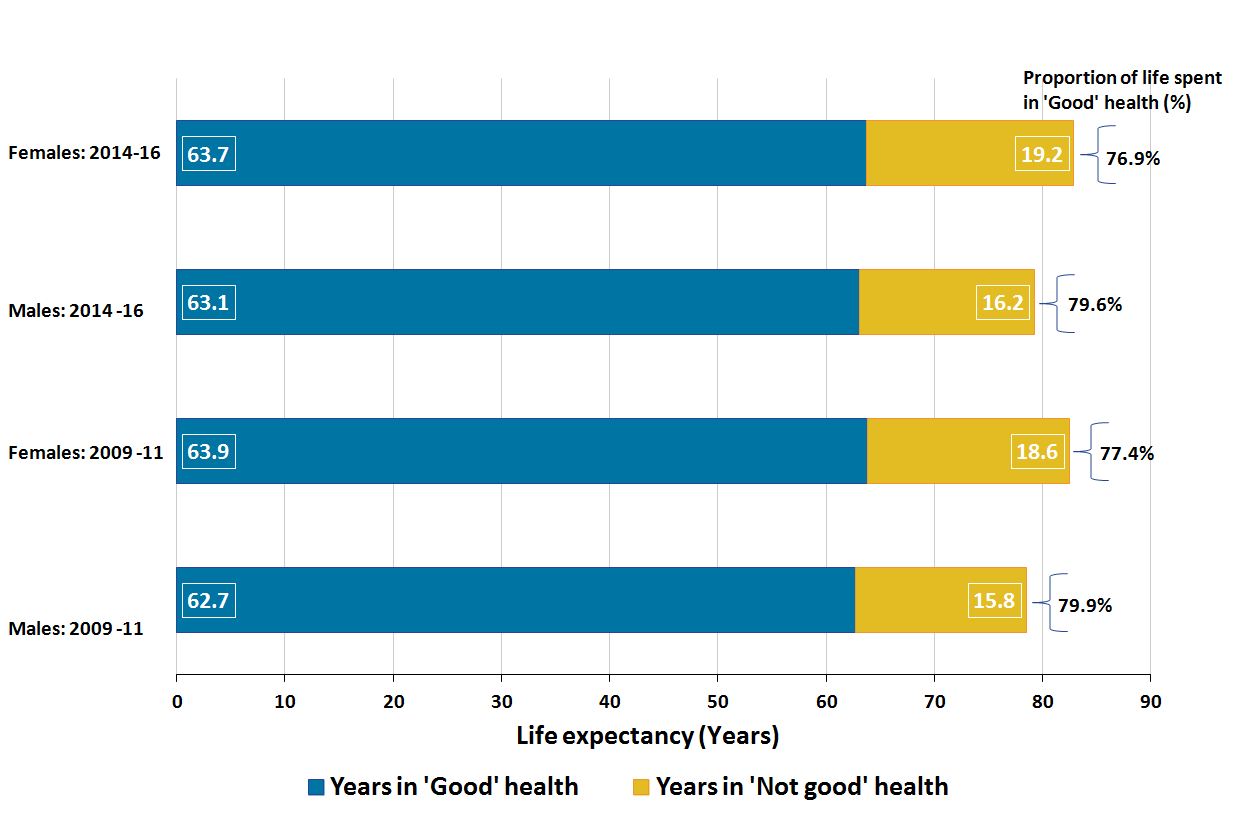{kind=link}
If the UK experienced the same self-reported health and mortality rates that were observed during 2014 to 2016, males could expect to live 63.1 years in good health (79.6% of their life) and females 63.7 years (76.9% of their life).
When compared with the earliest period 2009 to 2011, HLE at birth has increased by 0.4 years for males and reduced by 0.2 years for females. This has the effect of closing the gender gap in years lived in good health to 0.6 years from 1.1 years in 2009 to 2011. It also results in females living three years longer in a state of “not good health” than males because of longer female life expectancy. This has the consequence of females living a smaller proportion of their lives in “good” health in 2014 to 2016 compared with 2009 to 2011.
HLE and disability-free life expectancy (DFLE) across constituent countries in the UK between 2009 to 2011 and 2014 to 2016 can be accessed in the accompanying datasets. The trend in DFLE is not reported on because of one minor and one major change in the survey questions used to estimate disability in the Annual Population Survey (APS) between 2009 to 2011 and 2014 to 2016.
However, it is important to note that DFLE estimates for the period 2014 to 2016 are based on the latest harmonised standard questions exclusively for the first time. More information is available in the Health state life expectancies Quality and Methodology Information report.
Nôl i'r tabl cynnwys8. People living in Scotland spend the highest proportion of life in “good” health, despite having the lowest life expectancy
Life expectancy at birth for males in England was 2.4 years longer than in Scotland and half of these extra life years were spent in “good” health (Table 1). However, when seen in the context of the proportion of life spent healthy, because males in Scotland have a shorter life expectancy, they spend more of their life in good health and live fewer years in “not good” heath.
Table 1: Health state life expectancy at birth and at age 65 for males across constituent countries in the UK, 2014 to 2016
| Life expectancy (Years) | Healthy life expectancy (Years) | Years in 'Not good' health (Years) | Proportion of life expectancy (%) | Disability-free life expectancy (Years) | Years with disability (Years) | Proportion of life expectancy (%) | |||||||||
| At birth | |||||||||||||||
| England | 79.5 | 63.3 | 16.2 | 79.6 | 62.8 | 16.7 | 79.0 | ||||||||
| Wales | 78.4 | 61.6 | 16.9 | 78.5 | 59.9 | 18.5 | 76.4 | ||||||||
| Scotland | 77.1 | 62.2 | 14.8 | 80.7 | 61.8 | 15.3 | 80.1 | ||||||||
| Northern Ireland | 78.5 | 60.3 | 18.2 | 76.8 | 60.2 | 18.3 | 76.7 | ||||||||
| United Kingdom | 79.2 | 63.1 | 16.2 | 79.6 | 62.5 | 16.7 | 78.9 | ||||||||
| At age 65 | |||||||||||||||
| England | 18.8 | 10.5 | 8.2 | 56.0 | 10.0 | 8.7 | 53.5 | ||||||||
| Wales | 18.2 | 10.0 | 8.2 | 54.8 | 8.9 | 9.3 | 48.9 | ||||||||
| Scotland | 17.4 | 10.1 | 7.3 | 57.9 | 9.7 | 7.7 | 55.5 | ||||||||
| Northern Ireland | 18.3 | 9.3 | 9.0 | 50.6 | 9.4 | 8.9 | 51.2 | ||||||||
| United Kingdom | 18.6 | 10.4 | 8.2 | 56.0 | 9.9 | 8.7 | 53.4 | ||||||||
| Source: Office for National Statistics | |||||||||||||||
| Notes: | |||||||||||||||
| 1. Figures may not sum because of the rounding. | |||||||||||||||
Download this table Table 1: Health state life expectancy at birth and at age 65 for males across constituent countries in the UK, 2014 to 2016
.xls (29.7 kB)When looking at disability-free life expectancy (DFLE) at birth for males, disability-free life years were shortest in Wales (59.9 years) and longest in England (62.8 years), with a 2.9-year gap. Males in Wales were expected to live 18.5 years with a limiting long-term physical or mental health condition, whereas in England it was 16.7 years. Consequently, males in England not only have a longer life than males in Wales, they also spend a higher proportion of their lives disability-free (Table 1).
At birth, males across all countries spend a smaller proportion of their lives disability-free than in good health.
DFLE at age 65 is an important summary measure as it informs fitness for work after the current State Pension age of 65. DFLE was highest in England (10.0 years) and lowest in Wales (8.9 years). In both countries men can expect to live 8.7 years and 9.3 years respectively with a limiting long-term physical or mental health condition. Therefore, men in Wales are expected to spend less than half their remaining life disability-free.
Life expectancy at birth for females in England was two years longer than in Scotland and a quarter of these extra life years were spent in “good” health (Table 2). However, when seen in the context of the proportion of life spent healthy, because females in Scotland have a shorter life expectancy, they spend more of their life in good health and live fewer years in “not good” heath than females in England. In England, females were living 1.5 years longer in “not good” health than in Scotland.
Table 2: Health state life expectancy at birth and at age 65 for females across constituent countries in the UK, 2014 to 2016
| Life expectancy (Years) | Healthy life expectancy (Years) | Years in 'Not good' health (Years) | Proportion of life expectancy (%) | Disability-free life expectancy (Years) | Years with disability (Years) | Proportion of life expectancy (%) | ||||||||
| At birth | ||||||||||||||
| England | 83.1 | 63.9 | 19.3 | 76.8 | 62.3 | 20.8 | 75.0 | |||||||
| Wales | 82.3 | 62.7 | 19.7 | 76.1 | 59.3 | 23.1 | 72.0 | |||||||
| Scotland | 81.1 | 63.4 | 17.8 | 78.1 | 61.6 | 19.5 | 75.9 | |||||||
| Northern Ireland | 82.3 | 62.5 | 19.8 | 75.9 | 61.4 | 20.9 | 74.6 | |||||||
| United Kingdom | 82.9 | 63.7 | 19.2 | 76.9 | 62.1 | 20.8 | 74.9 | |||||||
| At age 65 | ||||||||||||||
| England | 21.1 | 11.3 | 9.8 | 53.4 | 10.2 | 10.9 | 48.3 | |||||||
| Wales | 20.6 | 10.7 | 9.8 | 52.2 | 9.0 | 11.5 | 44.0 | |||||||
| Scotland | 19.7 | 11.2 | 8.5 | 56.7 | 10.2 | 9.6 | 51.5 | |||||||
| Northern Ireland | 20.6 | 10.6 | 10.0 | 51.3 | 9.6 | 11.0 | 46.5 | |||||||
| United Kingdom | 21.0 | 11.2 | 9.7 | 53.6 | 10.1 | 10.8 | 48.4 | |||||||
| Source: Office for National Statistics | ||||||||||||||
| Notes: | ||||||||||||||
| 1. Figures may not sum because of the rounding. | ||||||||||||||
Download this table Table 2: Health state life expectancy at birth and at age 65 for females across constituent countries in the UK, 2014 to 2016
.xls (30.2 kB)When looking at DFLE at birth for females, disability-free life years were shortest in Wales (59.3 years) and longest in England (62.3 years), with a three-year gap. Females in Wales were expected to live 23.0 years with a limiting long-term physical or mental health condition, whereas in England it was 20.8 years. Consequently, females in England have a longer life than females in Wales and spend a higher proportion of their lives disability-free (Table 2).
At birth, females across all countries spend a smaller proportion of their lives disability-free than in good health.
For women at age 65, DFLE was highest in England and Scotland (10.2 years) and lowest in Wales (9.0 years). In Scotland, women can expect to live 9.5 years with a limiting long-term physical or mental health condition, whereas in Wales, it was 11.6 years. Women in Wales at age 65 could expect to spend only 44% of their remaining life disability-free.
Nôl i'r tabl cynnwys9. Healthy life expectancy at birth differs by 18 years across UK local areas
Across the UK in 2014 to 2016, healthy life expectancy (HLE) at birth was highest in the London borough of Richmond upon Thames for males (69.9 years) and the Orkney Islands for females (73.0 years). The lowest HLE was observed in Dundee City in Scotland for males (54.3 years) and in Manchester for females (54.6 years). The gap in HLE between local areas stands at 18.4 years for females and 15.6 years for males.
Areas with the highest and lowest HLE can be identified by looking at the top right and bottom left of Figures 8 and 9, which show the relationship between life expectancy and HLE.
Figure 8: Relationship between male healthy life expectancy and life expectancy at birth in local areas in the UK, 2014 to 2016
Source: Annual Population Survey, Office for National Statistics
Notes:
Local areas are 150 upper tier local authorities (UTLAs) in England, 22 unitary authorities in Wales, 32 council areas in Scotland and 11 local government districts in Northern Ireland.
Excluded areas are the Isles of Scilly and City of London because of small populations.
Areas with small populations, such as Orkney Islands, tend to have a wider confidence interval than areas with larger populations such as Essex.
Figures may not sum because of the rounding.
Download this chart Figure 8: Relationship between male healthy life expectancy and life expectancy at birth in local areas in the UK, 2014 to 2016
Image .csv .xls
Figure 9: Relationship between female healthy life expectancy and life expectancy at birth in local areas in the UK, 2014 to 2016
Source: Annual Population Survey, Office for National Statistics
Notes:
Local areas are 150 upper tier local authorities (UTLAs) in England, 22 Unitary Authorities in Wales, 32 Council Areas in Scotland and 11 Local Government Districts in Northern Ireland.
Excluded Isle of Scilly and City of London because of a sample size issue
Areas with small populations, such as Orkney Islands, tend to have wider confidence interval than areas with larger populations.
Figures may not sum because of the rounding.
Download this chart Figure 9: Relationship between female healthy life expectancy and life expectancy at birth in local areas in the UK, 2014 to 2016
Image .csv .xls10. Local area gap in years lived in good health exceeds 10 years among pensioners in the UK
As can be seen from Figures 10 and 11, there is a clear linear relationship between living longer and living longer in a state of good health. However, there are stark contrasts in the number of years that pensioners expect to spend in good health in the UK.
For instance, men in Dorset and Kingston upon Thames have a similar life expectancy, but healthy life expectancy (HLE) differs by 4.9 years (16.1 years in Kingston upon Thames and 11.2 years in Dorset).
For men, the largest absolute gap in HLE was 10.2 years between Kingston upon Thames and Manchester. For women, the equivalent gap was 9.5 years between the Orkney Islands and Tower Hamlets.
When benchmarking local area HLE with the national UK average, one-fifth of local areas had healthy life expectancy significantly higher than the UK.
Figure 10: Relationship between health state life expectancies at age 65 in the UK, men, 2014 to 2016
Source: Annual Population Survey, Office for National Statistics
Notes:
For men, 44 out of 215 local areas had healthy life expectancy significantly higher than the UK average (10.4 years).
Statistical significance was examined by one-tailed Z scores. Detailed information about this can be viewed in Appendix 1 of the Sullivan guide.
Local areas are 150 upper tier local authorities (UTLAs) in England, 22 unitary authorities in Wales, 32 council areas in Scotland and 11 local government districts in Northern Ireland.
Excluded areas are the Isles of Scilly and City of London because of small populations.
Areas with small populations, such as Orkney Islands, tend to have a wider confidence interval than areas with larger populations such as Essex.
Figures may not sum because of the rounding.
Download this chart Figure 10: Relationship between health state life expectancies at age 65 in the UK, men, 2014 to 2016
Image .csv .xls
Figure 11: Relationship between health state life expectancies at age 65 in the UK, women, 2014 to 2016
Source: Annual Population Survey, Office for National Statistics
Notes:
For women, 45 out of 215 local areas had healthy life expectancy significantly higher than the UK average (11.2 years).
Statistical significance was examined by one-tailed Z scores. Detailed information about this can be viewed in Appendix 1 of the Sullivan guide.
Local areas are 150 upper tier local authorities (UTLAs) in England, 22 unitary authorities in Wales, 32 council areas in Scotland and 11 local government districts in Northern Ireland.
Excluded areas are the Isles of Scilly and City of London because of small populations.
Areas with small populations, such as Orkney Islands, tend to have a wider confidence interval than areas with larger populations such as Essex.
Figures may not sum because of the rounding.
Download this chart Figure 11: Relationship between health state life expectancies at age 65 in the UK, women, 2014 to 2016
Image .csv .xlsFigure 12 shows healthy life expectancy at birth and age 65 for upper tier local authorities in England from 2009 to 2011 and 2014 to 2016. This provides the opportunity to compare the improvement in healthy life expectancy at important ages against the national average over time. This is restricted to England as historical estimates are not available for Scotland, Wales and Northern Ireland. This will be addressed following the outcome of the consultation when we intend to provide a back series for other local areas in the UK.
Figure 12: Healthy life expectancy at birth and age 65 by sex, England, 2009 to 2011 and 2014 to 2016
Embed code
11. Quality and methodology
The Health state life expectancies Quality and Methodology Information report contains important information on:
the strengths and limitations of the data and how it compares with related data
uses and users of the data
how the output was created
the quality of the output including the accuracy of the data
What are health state life expectancies?
Health state life expectancies add a quality of life dimension to estimates of life expectancy (LE) by dividing expected life span into time spent in different states of health or disability. Healthy life expectancy (HLE), which estimates lifetime spent in “Very good” or “Good” health, is based on how individuals perceive their general health. The second is disability-free life expectancy (DFLE), which estimates lifetime free from a limiting persistent illness or disability. This is based upon a self-rated assessment of how health conditions and illnesses limit an individual’s ability to carry out day-to-day activities.
Both health state life expectancies are summary measures of population health and important indicators of the well-being of society, providing context to the effects of policy changes and interventions at both national and local levels. Health state life expectancies are used across public, private and voluntary sectors, in the assessment of healthy ageing, fitness for work, monitoring health improvement, fairness in extensions to the State Pension age, pension provision and health and social care need.
Estimates provided in this release provide a snapshot of health status of populations in the UK, assuming mortality and health status observed in 2014 to 2016 remained constant over time. However, health status and mortality rates in national and local area populations may change in the future, due to changes in exposure to health risks and innovations in treatment of diseases affecting health. Therefore, the estimates reported in this bulletin are a guide to the number of years a specific area’s population will live in different health states.
The questions classifying individuals to activity limitation were changed in April 2013 following a review into how disability should be measured in national surveys. Primary harmonised standards for disability data collection and the production of statistical measures of disability (PDF, 136.03KB) are available.
More information about the question change can be seen in the QMI report. Due to this change and the change in the introductory paragraph of the disability section being re-worded in 2010, there has been a difference in the number of people reporting disabilities. Therefore, estimates either side of the discontinuity (before and after April 2013) should not be directly compared.
Changes in health state life expectancies over time can be assessed by comparing non-overlapping time periods. Therefore, estimates for 2014 to 2016 should not be compared with estimates for 2013 to 2015 or 2012 to 2014 for example, as they will contain some of the same survey respondents.
How do we calculate health state life expectancies?
In this bulletin, data were calculated using abridged life table methods (based on five-year age groups). Life expectancy (LE) has been calculated using the standard Chiang II abridged life table method. However, estimation of the variance, used to measure the statistical precision of life expectancy estimates, has undergone one important modification as the Chiang II method assumes zero variance for the final age group. To enable the calculation of a confidence interval for the final age group, the method developed by Silcocks and others (2001) has been used and further information is available in the methods paper published in 2016.
Figures for England, Wales, English regions, counties and local authorities exclude deaths of non-residents. However, Scotland includes non-usual residents who die in Scotland and do not have an area of residence within Scotland and imputation is used to assign the death to an area of “residence” (see Section 1.3.1 in the Healthy life expectancy: technical paper for more detail).
Northern Ireland also includes non-usual residents that are allocated to the place of death (see Life expectancy for Northern Ireland information paper and methodology guide for more detail).
The data used in calculating the general health and disability status were obtained from the Annual Population Survey (APS). They were aggregated over a three-year period to achieve sufficiently large sample sizes to enable meaningful statistical comparison at national and subnational level.
The prevalence of “Good” general health and disability-free among males and females resident in private households in England was compared across areas. HLE was then calculated using the Sullivan method, which combines prevalence data with mortality and mid-year population estimates (MYE) over the same period and geographical coverage to calculate estimates of life expectancy (LE), healthy life expectancy (HLE) and disability-free life expectancy by age and sex (for more information, see the ONS life table template).
The APS provides prevalence information for those aged 16 and over. We are able to estimate lower age groups by using a census imputation method.
Results are presented with 95% confidence intervals in reference tables to help interpretation. Confidence intervals in this statistical bulletin indicate the uncertainty surrounding health state life expectancy estimates and allow more meaningful comparisons between areas. Within this bulletin, a difference that is described as “significant” is statistically significant and has been assessed using the z-test. More information about this z-test can be viewed in Appendix 1 of the Sullivan guide.
What is the difference between the mean, median and modal age at death?
Average life spans are usually measured using the life table. A life table is a standard method of analysing mortality by age to summarise a population’s mortality experiences. These mortality experiences can be presented using three measures of average life span:
the mean
the median
the mode
Median and modal ages at death can be measured using period life tables as well. Period life tables use the current age-specific mortality rates with no assumption about the projected death rates. Therefore, age at death reported here for the given time period is the expected age at death if a person experienced those age-specific mortality rates throughout his or her life.
All three measures of life span are summary measures of ageing in a population, helping to understand mortality improvements over time. They feed into the policies surrounding pension provision and needs in the areas of housing and health and social care.
The mean
The most commonly used measure of average life span is life expectancy at birth or the mean age at death. It is the average number of years a person is expected to live before his or her death. We regularly produce period life expectancy, which is widely understood and used as a robust measure of population health.
The median
The second measure is the median age at death. This estimates the age at which half of a hypothetical cohort would have died and half would still be alive.
The mode
A third measure of life span is the late modal age at death. This measure, which has emerged as an alternative measure of life span in low infant mortality countries such as UK, identifies the age at which the highest number of deaths occur over the life course. This focuses on deaths occurring at older ages in the life table in its calculation.
How it is calculated
Mean age at death (life expectancy at birth) is calculated using the standard Chiang II methods for the abridged life table, where the final age band was closed at age 95 and over to measure the survival at older ages.
In the abridged life table, median and modal age groups are identified using the dx column in the life table, which represents the expected number of deaths in each age group based on the probability of dying in the specific age interval in a hypothetical cohort of 100,000 persons.
By using dx, the modal age group is where the highest number of deaths occurred out of this cohort of 100,000; the median age group is where cumulative deaths (that is, dxi plus dx(i-1)) exceed 50,000. After identifying the median and modal age groups, group data formulas are applied to obtain approximate median and modal ages at death.
Nôl i'r tabl cynnwys