1. Main points
There was a statistically significant change in the pattern of all-cause daily deaths in England and Wales that occurred on 18 March 2020 with the rate of change increasing from an increase of 0.8 deaths on average per day to an increase of 73.5 deaths on average per day reaching a peak on 8 April; the rate of change in the number of deaths then declined steeply until 11 May.
Looking at coronavirus (COVID-19) mortality, the significant change in trend started on 20 March, from which date deaths involving COVID-19 increased by an average of 68.4 deaths per day until 8 April before falling again, following a very similar pattern to all-cause deaths.
Non-COVID-19 mortality followed a slightly different pattern to COVID-19 and all-cause mortality; non-COVID-19 deaths peaked a few days later on 11 April and declined steeply until 10 May, then increased gradually thereafter.
This analysis adds to previous knowledge by indicating exactly when statistically significant changes in the trends in daily deaths occurred; the dates highlighted are not designed to define when one wave of the pandemic started or finished.
The fact that non-COVID-19 deaths peaked at a similar time to COVID-19 deaths supports the possibility that excess non-COVID-19 deaths in the earlier months may have been caused directly by undiagnosed COVID-19; in contrast, in the later months the slight increase in non-COVID-19 deaths might be attributed to indirect consequences of the pandemic such as delayed care.
The peak in all-cause and COVID-19 mortality occurred at similar times in private homes (4 April) and hospitals (7 April) but peaked later in care homes (12 April); this could indicate different patterns of infection in the different settings.
2. Changes in mortality in 2020
2019 saw the first year-on-year decrease in the number of deaths since 2016 and had the lowest annual age-standardised mortality rate recorded since our data time series began in 1994. The first few months of 2020 continued the trend of low mortality, with the majority of deaths recorded each week falling below the five-year average (2015 to 2019), which in part can be explained by the mild winter in 2019 to 2020 (PDF, 439KB) and low levels of circulating influenza (PDF, 2.2MB). This changed when coronavirus (COVID-19) deaths began to be registered in March 2020, leading to a steep rise in both all-cause and COVID-19 deaths.
We have reported regularly on the time trends of deaths in the pandemic period since March, in our deaths registered weekly (numbers of deaths) and monthly mortality analysis (age-standardised mortality rates) publications. Patterns over time in non-COVID-19 deaths and international comparisons have also been published. In this bulletin, we identify exactly when statistically significant changes in the mortality trends occurred, using a method called segmented breakpoint analysis.
This method (described in detail in Measuring the data) identifies the days when the rate of death changed significantly and determines the number of significant dates or "breakpoints" to look for in each data series; these are then derived from the data. Seasonal adjustment based on a five-year average was used to take into account the changes in mortality that are usually seen over the year.
Embed code
All-cause mortality
Figure 1: The first significant change (breakpoint) in all-cause mortality occurred on 18 March
Number of deaths per day, all causes: England and Wales, deaths occurring between 28 December 2019 and 4 September 2020 and registered by 3 October 2020
Source: Office for National Statistics – Changes in all-cause and COVID-19 mortality over time: England and Wales
Notes:
- Figures include deaths of non-residents.
- Based on date of death, registered up to 3 October 2020.
- All figures for 2020 are provisional.
- Information on segmented regression, breakpoints and modelled deaths can be found in the measuring the data section.
- Modelled number of deaths based on fitting to seasonally adjusted deaths by date as provided by the segmented regression model.
Download this chart Figure 1: The first significant change (breakpoint) in all-cause mortality occurred on 18 March
Image .csv .xlsAs Figure 1 shows, the number of deaths day by day tends to be volatile. Using a seasonally adjusted daily mortality model, we applied segmented regression analysis to find out at which points over the period the trend in mortality changed statistically significantly.
The general distribution can be described by the following main changes.
On 28 December 2019 (the start of the year 2020 in terms of weekly mortality reporting) the number of deaths that occurred was 1,706; deaths rose to a peak of 3,241 on 8 April 2020 before decreasing to 1,270 deaths on 4 September. As this analysis is based on the date a death occurred rather than when it was registered, we expect the total recorded number of deaths to increase as more deaths are registered, especially for the most recent dates. This would be unlikely to alter the general distribution of mortality over the period.
Using four breakpoints, we can look more closely at where there were significant changes in the number of deaths per day.
Table 1 shows the date of each breakpoint calculated, the seasonally adjusted modelled number of deaths on that date, and the rate of increase or decrease in average deaths per day up to and from that breakpoint (rate of change).
| Breakpoint 1 | Breakpoint 2 | Breakpoint 3 | Breakpoint 4 | |
|---|---|---|---|---|
| Breakpoint (day) | Day 82: 18 March 2020 | Day 103: 8 April 2020 | Day 136: 11 May 2020 | Day 172: 16 June 2020 |
| Modelled deaths | 1,404 | 2,910 | 1,659 | 1,398 |
| Rate of change | +0.8/+73.5 | +73.5/-37.9 | -37.9/-7.4 | -7.4/-0.2 |
Download this table Table 1: Breakpoints in rate of change for all-cause mortality
.xls .csvBetween 28 December 2019 and 18 March 2020, the number of all-cause deaths rose by 0.8 deaths per day on average. We then saw a statistically significant change in the pattern of daily deaths with an increase of 73.5 deaths on average per day until 8 April, the peak of the coronavirus pandemic. The average number of deaths per day decreased by 37.9 deaths per day until 11 May, then decreased at a slower rate of 7.4 deaths per day until 16 June, followed by a very small rate of further decrease at 0.2 deaths per day.
COVID-19 mortality
The main driver of mortality over the period March to June was COVID-19. Looking at COVID-19 specifically, we see slightly different dates where the mortality trend changed, compared with the all-cause mortality.
We use the term "due to COVID-19" when referring only to deaths with an underlying cause of death of COVID-19, and we use the term "involving COVID-19" when referring to deaths that had COVID-19 mentioned anywhere on the death certificate, whether as an underlying cause or not. The following analysis will focus on all deaths involving COVID-19.
Figure 2: The first significant change (breakpoint) in all-cause mortality occurred on 20 March
Number of deaths per day, deaths involving COVID-19, England and Wales, deaths occurring between 28 December 2019 and 4 September 2020 and registered by 3 October 2020
Source: Office for National Statistics – Changes in all-cause and COVID-19 mortality over time: England and Wales
Notes:
- Figures include deaths of non-residents.
- Based on date of death, registered up to 3 October 2020.
- All figures for 2020 are provisional.
- The International Classification of Diseases, 10th edition (ICD-10) definitions are as follows: coronavirus (COVID-19) (U07.1 and U07.2).
- Information on segmented regression, breakpoints and modelled deaths can be found in the measuring the data section
- Modelled number of deaths based on fitting to seasonally adjusted deaths by date as provided by the segmented regression model.
Download this chart Figure 2: The first significant change (breakpoint) in all-cause mortality occurred on 20 March
Image .csv .xls
| Breakpoint 1 | Breakpoint 2 | Breakpoint 3 | Breakpoint 4 | |
|---|---|---|---|---|
| Breakpoint (day) | Day 84: 20 March 2020 | Day 103: 8 April 2020 | Day 136: 11 May 2020 | Day 172: 16 June 2020 |
| Modelled deaths | 37 | 1,297 | 399 | 76 |
| Rate of change | +0.4/+68.4 | +68.4/-28.2 | -28.2/-9.1 | -9.1/-1 |
Download this table Table 2: Breakpoints in rate of change for COVID-19 mortality
.xls .csvA similar pattern of changes in the mortality trend can be seen in COVID-19 mortality as in all-cause mortality. The significant changes happened on the same dates, but some of the rates of change differed slightly compared with all-cause mortality. Deaths involving COVID-19 increased at a rate of 0.4 deaths per day on average until 20 March where they started to increase on average by 68.4 deaths per day until 8 April, a similar pattern to that seen in all-cause mortality.
The number of deaths then decreased by 28.2 deaths per day until 11 May, 9.1 deaths per day until 16 June and 1.0 death per day from then on. This is a slightly slower pattern of decline in daily deaths compared with the 37.9, 7.4 and 0.2 average decreases in deaths per day seen in all-cause mortality for those periods.
Non-COVID-19 mortality
As stated previously, the main change in the mortality trend was COVID-19. This explains why the pattern for non-COVID-19 deaths differs more than COVID-19 deaths from the pattern seen in all-cause mortality. The segmented regression analysis looking at non-COVID-19 mortality identified only two statistically significant breakpoints in the data time series.
More information on the methodology can be found in Measuring the data.
Figure 3: Unlike all-cause and COVID-19 mortality, there were only two breakpoints in non-COVID-19 mortality
Number of deaths per day, deaths not involving COVID-19, England and Wales, deaths occurring between 28 December 2019 and 4 September 2020 and registered by 3 October 2020
Source: Office for National Statistics – Changes in all-cause and COVID-19 mortality over time: England and Wales
Notes:
- Figures include deaths of non-residents.
- Based on date of death, registered up to 3 October 2020.
- All figures for 2020 are provisional.
- Information on segmented regression, breakpoints and modelled deaths can be found in the measuring the data section.
- Modelled number of deaths based on fitting to seasonally adjusted deaths by date as provided by the segmented regression model.
Download this chart Figure 3: Unlike all-cause and COVID-19 mortality, there were only two breakpoints in non-COVID-19 mortality
Image .csv .xls
| Breakpoint 1 | Breakpoint 2 | |
|---|---|---|
| Breakpoint (day) | Day 106: 11 April 2020 | Day 135: 10 May 2020 |
| Modelled deaths | 1,526 | 1,277 |
| Rate of change | +2.4/-8.6 | -8.6/+1 |
Download this table Table 3: Breakpoints in rate of change for non-COVID-19 mortality: England and Wales, deaths occurring between 28 December 2019 and 4 September 2020 and registered by 3 October 2020
.xls .csvFor deaths not involving COVID-19, the number of deaths per day increased by 2.4 deaths per day on average until 11 April; from then on the number of deaths per day decreased by an average of 8.6 deaths per day until 10 May, when it started to increase by 1.0 death per day until the end of the period covered. Although there were only two breakpoints in non-COVID-19 mortality, these were at similar times to the all-cause and COVID-19 breakpoint 2 and 3 dates respectively, but the rate of change and direction of change differed.
Figure 4: There were two breakpoints in non-COVID-19 mortality, at similar times to the all-cause and COVID-19 breakpoint 2 and 3 respectively, but the rate and direction of change differed
Modelled number of deaths per day, by cause, England and Wales, deaths occurring between 28 December 2019 and 4 September 2020 and registered by 3 October 2020
Source: Office for National Statistics – Changes in all-cause and COVID-19 mortality over time: England and Wales
Notes:
- Figures include deaths of non-residents.
- Based on date of death, registered up to 3 October 2020.
- All figures for 2020 are provisional.
- Information on segmented regression, breakpoints and modelled deaths can be found in the measuring the data section
- Modelled number of deaths based on fitting to seasonally adjusted deaths by date as provided by the segmented regression model.
Download this chart Figure 4: There were two breakpoints in non-COVID-19 mortality, at similar times to the all-cause and COVID-19 breakpoint 2 and 3 respectively, but the rate and direction of change differed
Image .csv .xlsSmoothing out the day-to-day variation in deaths using segmented regression analysis gives a clear and objective picture of how and when the trends in deaths changed over time. While the breakpoints can be seen as simply delineating the previously observed shape of the large excess of deaths in April and May 2020, Figure 4 illustrates how some specific points of interest are identified by the differences breakpoints and rates of change described in Table 3 compared with Tables 1 and 2.
The trend in COVID-19 mortality is largely similar to that of all-cause mortality, likely because of the large number of deaths attributed to that cause over the period of interest. Although all-cause mortality and deaths involving COVID-19 both identified four changes in the mortality trend, while deaths not involving COVID-19 identified only two breakpoints, all three measures agree that a change in the mortality trend occurred around the middle of April and again in the middle of May.
The fact that non-COVID-19 deaths peaked at the same time as COVID-19 deaths suggests that a proportion of non-COVID-19 deaths in the earlier months may in fact have been caused directly by undiagnosed COVID-19. Diagnosis of COVID-19 at the beginning of the period is likely to have been affected by the lack of tests and the limited information available at that time on transmission, symptoms and pathological features. From our analysis on deaths registered weekly in England and Wales, the earliest date of a death involving COVID-19 known so far is in the week ending 31 January 2020.
However, the subsequent gradual increase in non-COVID-19 deaths while COVID-19 deaths fell may suggest a different pattern, possibly including the effects of delayed or interrupted treatment for other health conditions. Our previous analysis on deaths not involving the coronavirus provides more information on potentially undiagnosed COVID-19 and deaths that may be indirectly due to COVID-19.
Analysis split by sex is available in the accompanying dataset. An interesting finding when looking at males and females separately can be found when looking at non-COVID-19-related deaths. For males, any changes over time are subtle, however deaths of females show a clear peak and three breakpoints. A possible reason for this difference is that the pattern of non-COVID-19 mortality in males shows evidence of mortality displacement (where a large number of people died earlier in the year, reducing the number of people in the same group who died in later months).
The pattern in females could be linked to the breakpoint analysis findings on care homes (reported in Section 3) as there tend to be more females in care homes than males. Our deaths in the care sector release reported that females represent a larger proportion of care home residents than males and that a lower mortality rate is expected among female care home residents because, on average, women are living longer than men. It is estimated that there are more females in the care home resident population; in our estimates, females account for 66.5% of the care home resident population in England and 67.2% of the care home resident population in Wales.
Nôl i'r tabl cynnwys3. Differences in time trends by place of death
This section focuses on all-cause mortality in hospitals, care homes and private homes. More detailed information on coronavirus (COVID-19) and non-COVID-19 mortality can be found in the accompanying dataset.
Figure 5: Deaths in private homes and hospitals peaked earlier than those in care homes
Number of modelled deaths per day, all causes, by place of death, England and Wales, deaths occurring between 28 December 2019 and 4 September 2020 and registered by 3 October 2020
Source: Office for National Statistics – Changes in all-cause and COVID-19 mortality over time: England and Wales
Notes:
- Figures include deaths of non-residents.
- Based on date of death, registered up to 3 October 2020.
- All figures for 2020 are provisional.
- Information on segmented regression, breakpoints and modelled deaths can be found in the measuring the data section.
- Modelled number of deaths based on fitting to seasonally adjusted deaths by date as provided by the segmented regression model.
- Based on place a death occurred.
Download this chart Figure 5: Deaths in private homes and hospitals peaked earlier than those in care homes
Image .csv .xls
| Breakpoint 1 | Breakpoint 2 | Breakpoint 3 | Breakpoint 4 | ||
|---|---|---|---|---|---|
| Hospital | Breakpoint (day) | Day 79: 15 March 2020 | Day 102: 07 April 2020 | Day 125: 30 April 2020 | Day 169: 13 June 2020 |
| Rate of change | 0.0/+27.5 | +27.5/-23.5 | -23.5/-3.2 | -3.2/+0.3 | |
| Care home | Breakpoint (day) | Day 87: 23 March 2020 | Day 107: 12 April 2020 | Day 137: 12 May 2020 | Day 163: 07 June 2020 |
| Rate of change | +0.4/+34.4 | +34.4/-17.6 | -17.6/-6.2 | -6.2/-0.1 | |
| Home | Breakpoint (day) | Day 81: 17 March 2020 | Day 99: 04 April 2020 | Day 136: 11 May 2020 | |
| Rate of change | +0.3/+14.2 | +14.2/-4.8 | -4.8/-0.4 |
Download this table Table 4: Breakpoint analysis summary by place of death, all-cause mortality, England and Wales, deaths occurring between 28 December 2019 and 4 September 2020 and registered by 3 October 2020
.xls .csvAs can be seen in Table 4, breakpoints differ when looking across different places of death. The earliest breakpoint in the rate of change for all-cause deaths can be seen for deaths occurring in hospital. At the start of the coronavirus pandemic, the majority of COVID-19 deaths occurred in hospital, which explains this earlier change. The number of deaths in hospitals was stable until 15 March 2020 when it started to increase on average by 27.5 deaths per day until 7 April.
This increasing rate results from a combination of a sharper increase in the rate of COVID-19 deaths per day in hospitals (which increased at 47.7 deaths per day from a modelled 17 deaths on 19 March to 921 modelled deaths on 7 April) and a decrease in the non-COVID-19 hospital death rate (falling at a rate of 19.7 deaths per day from 621 modelled deaths on 23 March to 301 modelled deaths on 8 April).
From 7 April, the all-cause death rate decreased by 23.5 deaths per day on average in hospitals until 30 April. From 30 April, the number of deaths per day decreased by 3.2 deaths per day on average until 13 June where it started to rise again by 0.3 deaths per day on average.
Looking at deaths that occurred in care homes, the first breakpoint occurred later in the data time series, on 23 March 2020, when the average daily rise in deaths increased sharply from 0.4 deaths per day to 34.4 deaths per day. This is made up of increases in the rate of both non-COVID-19 deaths (increasing at 16.8 deaths per day from 19 March) and COVID-19 deaths (an increase of 20.5 deaths per day beginning over a week later on 28 March).
The non-COVID-19 deaths in care homes peaked on 8 April at a modelled rate of 646 deaths per day before falling by 11.1 deaths per day to 11 May. In contrast, the COVID-19 deaths in care homes peaked on 16 April at 399 deaths per day before falling by 8.6 deaths per day to 21 May.
These trends combined to create the three further all-cause death rate breakpoints occurring on 12 April, 12 May and 7 June when the number of all-cause deaths per day decreased on average by 17.6, 6.2 and 0.1 deaths per day respectively.
These patterns reflect a somewhat later trend in care homes compared to hospital deaths, and also an increase in non-COVID-19 care home deaths that may include both undiagnosed COVID-19 and also patients with chronic or terminal illness who would more usually have died in hospital. The slower rate of decline in the pandemic in care homes may also reflect multiple outbreaks among the highly vulnerable care home population.
For all-cause deaths at home, the first breakpoint can be seen a couple of days later than for deaths occurring in hospitals. The first change in rate occurred on 17 March when deaths per day changed from increasing by 0.3 deaths per day on average to increasing sharply by 14.2 deaths per day. This was largely driven by an increase in the non-COVID-19 death rate of 9.8 per day from 355 deaths on 15 March to 547 deaths on 4 April.
This corresponds to the peak of the COVID-19 death rate in private homes that reached 69 per day on 4 April. Thereafter, the all-cause death rate decreased by 4.8 deaths per day on average before decreasing at a slower rate of 0.4 deaths per day on average from 11 May. Again, this change was largely driven by non-COVID-19 deaths, the rate of which fell at 3.2 deaths per day to 11 May.
Unlike deaths in hospitals and care homes, there were only three breakpoints identified for private homes. The number of deaths in private homes has been above average for the majority of 2020.
Further analysis of these deaths can be found in our Deaths in private homes release. While the number of COVID-19 deaths in private homes was not as great as was seen in hospitals and care homes, there have been substantial numbers of non-COVID-19 deaths at home throughout the year.
Nôl i'r tabl cynnwys4. Mortality data
Changes in all-cause and COVID-19 mortality over time, England and Wales
Dataset | Released 18 December 2020
Analysis of all-cause mortality and deaths involving COVID-19 using segmented regression.
5. Glossary
Coronaviruses
The World Health Organization (WHO) defines coronaviruses as "a large family of viruses that are known to cause illness ranging from the common cold to more severe diseases such as Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS)". Between 2001 and 2018, there were 12 deaths in England and Wales due to a coronavirus infection, with a further 13 deaths mentioning the virus as a contributory factor on the death certificate.
Coronavirus (COVID-19)
COVID-19 refers to the "coronavirus disease 2019" and is a disease that can affect the lungs and airways. It is caused by a type of coronavirus. Further information is available from the World Health Organisation (WHO).
Registration delay
Mortality statistics are compiled from information supplied when deaths are certified and registered as part of civil registration, a legal requirement. According to the Births and Deaths Registration Act 1953, a death should be registered within five days unless it is referred to a coroner for investigation. Mortality statistics for a given time period can be based on occurrence (death date) or registration (registration date); registration delay is the difference between date of occurrence and date of registration.
Statistical significance
The term "significant" refers to statistically significant changes or differences. Significance has been determined using the 95% confidence intervals, where instances of non-overlapping confidence intervals between estimates indicate the difference is unlikely to have arisen from random fluctuation. In some circumstances, significance has also been tested using z scores. More information about this z test is available in Appendix 1 of the Sullivan guide (PDF, 1.19MB).
Nôl i'r tabl cynnwys6. Measuring the data
Data used
The figures represent the number of deaths that occurred and were registered by 3 October 2020; a proportion of deaths occurring in this year will not be registered until subsequent years (more information can be found in our Impact of registration delays release).
Segmented regression approach
We used a segmented linear regression method to assess whether there has been a statistically significant change in the trend in mortality rates, and if so, at what point in the time series it moves away from the previous trend trajectory. Segmented linear regression fits multiple linear regression models to a series of continuous data to determine a trend using a segmented or broken line of best fit. The point at which one segment meets the next is called a breakpoint and indicates the point of a change in trend where the difference in the coefficients of the slopes before and after the breakpoint is statistically significant.
The segmented model produced is continuous so that the end of one segment must meet where the next segment begins. Linear models were chosen for simplicity and provide a sufficient approximation for this analysis.
We implemented this analysis using an algorithm in the software package R, the theory of which is explained in Segmented: An R Package to Fit Regression Models With Broken-Line Relationships. The "segmented" function in R allows users to specify the number of break points they wish to find. We initially set the function to detect one breakpoint, as we are testing for only one change in trend in our data time series.
The breakpoints found by the segmented function are the optimal points where linear models before and after the breakpoint have a greater goodness of fit than one model for the whole series. Goodness of fit statistics are provided with the accompanying dataset.
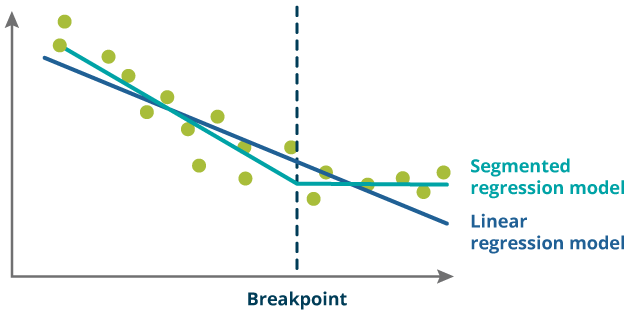
As shown in the schematic diagram (Figure 6), the orange line is a single linear regression model produced to fit all of the data (blue dots). The green line is a segmented regression model produced to fit the data assuming there is one breakpoint in the data. Overall, the green line fits the data much better than the orange line with many more blue data points being closer to the green line than the orange line.
The dashed black line shows where the change in trend (breakpoint) occurred. The exact position of this breakpoint does not precisely locate any source of change but can be used to see whether there is consistency across different countries, sexes and age groups about where the change in trend occurred in the data time series.
Figure 6: Schematic diagram of a segmented regression analysis
Source: Office for National Statistics
Download this image Figure 6: Schematic diagram of a segmented regression analysis
.png (24.2 kB)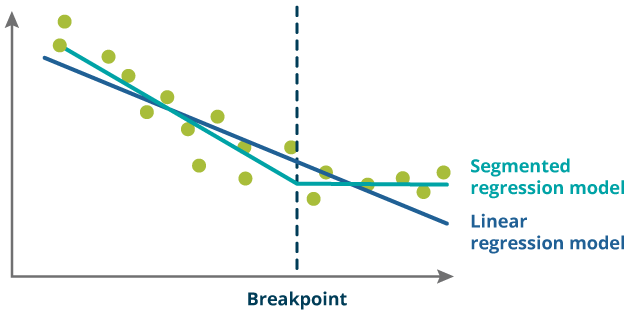{kind=link}
More quality and methodology information on strengths, limitations, appropriate uses, and how the data were created is available in the Mortality statistics in England and Wales QMI and the User guide to mortality statistics.
For each breakdown, the segmented regression model was run on seasonally adjusted data. Each model was run with one, two, three, four and five breakpoints. We then used the R squared value to determine which number of breakpoints best fit the data.
Nôl i'r tabl cynnwys7. Strengths and limitations
Strengths
Coding for cause of death is carried out according to the World Health Organization (WHO) ICD-10 and internationally agreed rules.
Information is supplied when a death is registered, which gives complete population coverage and ensures the estimates are of high precision, and representative of the underlying population at risk.
Limitations
The breakpoint is found using an iterative process, and so the exact breakpoint found may vary each time that a model is run. However, confidence intervals have been calculated to indicate the level of uncertainty around each breakpoint.
Deaths used in this analysis are based on deaths occurring in a certain period. Some deaths that have occurred in 2020 may not have been registered by the registration cut-off date and will not be included in this analysis. More information can be found in our Impact of registration delays release.
Nôl i'r tabl cynnwys