Cynnwys
- Introduction
- Main points
- Things you need to know about this release
- The new adult social care productivity measure
- Why methods changes are necessary
- Measuring inputs
- Measuring quantity output
- Quality adjustment
- Analysis of the new adult social care productivity series
- Adult social care productivity for England on financial year basis
- Additional adult social care productivity measures on an England financial year basis
- Acknowledgments
- References
- Links to related publications
1. Introduction
This article introduces improvements to the measure of public service productivity for adult social care, which are proposed to be implemented in the next edition of the annual publication: Public service productivity estimates: total public service, UK. The article will explain changes made to inputs and output measures, introduce a new quality adjustment for output and analyse the results of the new measure. In addition to a new productivity measure produced on the existing UK calendar year basis, this report also includes new measures produced on an England-only financial year basis, with separate measures for different service types.
Nôl i'r tabl cynnwys2. Main points
Improvements to inputs include improvements to the data source for NHS funding and improvements to the deflators.
Improvements to output include a new output index for 2014 onwards and the incorporation of output coverage for services where activity data are not available, such as direct payments.
A new quality adjustment is added, applying the concept of adjusted social care-related quality of life and data from the Adult Social Care Survey.
The new UK adult social care productivity measure fell by an average of 0.7% per year between 1997 and 2016.
Within this, the quality adjustment adds 0.8% per year on average to adult social care productivity growth since its introduction in 2010.
New measures for England show smaller falls in the productivity of services for adults aged over 65 years than for services for adults aged under 65 years between financial year ending 1997 and financial year ending 2011; while the productivity of services for both client groups is relatively stable between financial year ending 2011 and financial year ending 2017.
3. Things you need to know about this release
Public service productivity is estimated by comparing growth in the total quantity of output provided with growth in the total quantity of inputs used. If the growth rate of output exceeds the growth rate of inputs, productivity increases, meaning that more output is being produced for each unit of input. Conversely, if the growth rate of inputs exceeds the growth rate of output, then public service productivity will fall, indicating that less output is being produced for each unit of input.
Inputs are composed of labour, goods and services, and consumption of fixed capital, and are measured on a volume basis using deflated expenditure. Quantity output is measured as the number of individual activities performed, where activity data are available. Where activity data are not available, output is measured using the equivalent deflated expenditure data as inputs. A quality adjustment is introduced in this publication and applied to output to account for changes in service quality.
Whilst these productivity estimates provide a measure of the amount of output that is produced for each unit of input, they do not measure value for money, whether inputs have been obtained for the lowest possible cost, or the wider performance of public services.
This publication focuses on adult social care (ASC). ASC services provide care and support to older people, adults with learning or physical disabilities, adults with mental health problems, drug and alcohol misusers, and carers. Provision of ASC is the responsibility of local authorities in Great Britain.
ASC services include:
placements in residential and nursing care
provision of home care services
day care services
supported living and accommodation
“meals on wheels”
equipment and home adaptations
care assessments and support services
This article does not analyse or introduce changes to the measurement of productivity for children’s social care services, although these are also included in the public service productivity statistics.
While much of the data used in the measure are shared with the national accounts, methodological changes mean that both output and inputs in this publication are inconsistent with the national accounts, although the new activity data source and relevant methods changes will be incorporated into the national accounts in future.
We intend to incorporate the changes to the ASC productivity measure in the next edition of the annual Public service productivity estimates series, due to be published in January 2019. As part of the incorporation of the new ASC productivity estimates into the total public service productivity measure, further changes may be made and so these estimates should be regarded as experimental. We welcome feedback from users, which can be sent to james.lewis@ons.gov.uk.
An accompanying article alongside this release establishes the procedure for incorporating these changes into total public service productivity.
Nôl i'r tabl cynnwys4. The new adult social care productivity measure
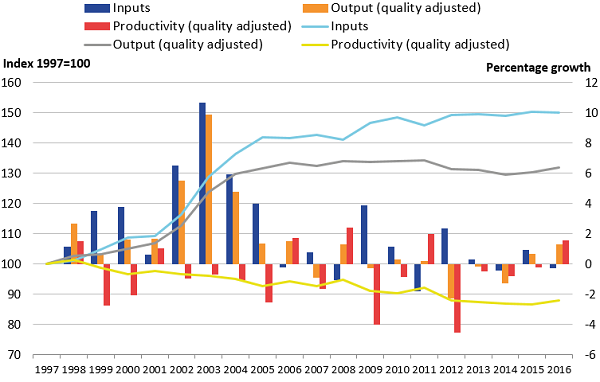
Figure 1 shows the new adult social care productivity series following the incorporation of methods improvements detailed in sections 5 to 8 of this article. Figure 1 shows public service adult social care productivity fell at an average annual rate of 0.7% over the period 1997 to 2016.
Figure 1: Public service adult social care inputs, and quality adjusted output and productivity indices
UK, 1997 to 2016
Source: Office for National Statistics
Notes:
- Quality adjustment applies from 2010 onwards.
Download this image Figure 1: Public service adult social care inputs, and quality adjusted output and productivity indices
.png (59.6 kB) .xls (34.8 kB){kind=link}
The chart also shows the trends in inputs and output growth over the same period. These show falls in productivity prior to 2005 were generally because of growth in inputs exceeding growth in output. Inputs and output have experienced smaller changes since 2005 and productivity in 2016 was at the same level as in 2012. The quality adjustment is introduced from 2010 onwards and has a positive effect on output and productivity for each year since its introduction.
Figure 2 illustrates how the new measure of public service adult social care productivity differs from the estimates previously published in Public service productivity estimates: total public service, UK: 2015. As a result of these changes, productivity has fallen more slowly than it had in the previously published series, particularly in 2012, where a reclassification that moved some housing spending into the inputs resulted in a fall in productivity in the previously published measure.
Figure 2: Public service adult social care productivity; comparison between new and previously published measures
UK, 1997 to 2016
Source: Office for National Statistics
Download this chart Figure 2: Public service adult social care productivity; comparison between new and previously published measures
Image .csv .xls5. Why methods changes are necessary
As a result of the introduction by NHS Digital of a new data collection for adult social care (ASC) activity in England, a new output index for England is required for financial year ending 2015 onwards. As the range of services covered by the new data collection is smaller than in the old collection, changes have been made to ASC output to include services for which activity data are not available, on an “output-equals-inputs” basis. This “output-equals-inputs” element has been implemented throughout the series back to 1997.
In addition, the existing output measure is not explicitly adjusted for quality. The Atkinson Review: Final report (PDF, 1.1MB), which determined the framework for public service productivity measurement, advised that where possible, changes in the quality of public service delivery should be considered to take account of changes in the value of services that are not captured through measuring changes in the quantity of output. Among other changes, this article introduces a quality adjustment, which is described in Section 8.
Developments in health and social care policy designed to generate better co-ordination between the NHS and local authority-provided ASC services, such as the introduction of the Better Care Fund in financial year ending 2016, have resulted in funding from the NHS making up an increasing proportion of ASC spending over time. To ensure the ASC productivity measure reflects these changes, improvements have been made to the measurement of NHS funding in both inputs and output1.
Finally, modifications have been made to the processing to enable the production of a financial year productivity measure for England. Processing now takes place on a financial year basis, with data converted to a calendar year basis at the end of the process, using the latest national accounts standards2, to produce the UK calendar year measure.
Notes for: Why methods changes are necessary
We intend to adjust the weights for adult social care and healthcare services, which are used to combine services in the measure of total public service productivity. An accompanying article released today (1 June 2018) provides more information on how methods changes will be incorporated in future total public service productivity articles.
To convert financial year data into calendar year, a technique known as cubic splining splits annual financial year volume or spending data into quarterly data, which are then re-aggregated to create calendar year figures. In this publication, the method used has been updated from X-11 ARIMA to X-13 ARIMA in line with latest national accounts practices. X-13 ARIMA has improved methods for forecasting and backcasting data as well as interpolating a trend within a data series.
6. Measuring inputs
Adult social care (ASC) inputs are estimated by deflating expenditure using appropriate deflators to convert current expenditure into a quantity input measure, alternatively known as a volume input measure. Changes in inputs can therefore result from both changes to expenditure and changes to the deflator used.
Local authority expenditure on adult social care
Public service adult social care is primarily funded by local authorities (LAs) in Great Britain. The LA current expenditure data used in the ASC productivity measure are part of the measure of social protection expenditure used in the national accounts. These national accounts data in turn are produced using the Local authority revenue expenditure and financing data return for England and equivalent data sources for Scotland1 and Wales. LA capital consumption2 is also measured using data from the national accounts and is estimated using the perpetual inventory method.
Data for LA current expenditure and capital consumption were used in the previously published public service ASC productivity estimates, and continue to be used in the latest estimates, with modifications to the current expenditure data explained in the following section.
It should be noted that, to analyse the productivity of specific services within ASC for England only, a different, more detailed data source is used for the new England financial-year ASC productivity measure and more details on this can be found in Section 10.
Due to a lack of inputs and output data, measures for Northern Ireland are not included in the ASC productivity estimates.
Changes to local authority expenditure – removal of housing services
Following changes made to the national accounts for Blue Book 2017, ASC expenditure also included local government expenditure on some housing services and on social protection not elsewhere classified from financial year ending 2012 (FYE 2012), resulting in more expenditure being included in the ASC inputs for the years 2012 onwards.
In the new ASC input measure, these changes are reversed, so that expenditure on housing and on social protection not elsewhere classified are excluded.
Change of source for NHS funding
In addition to funding from LAs, ASC services are also partly funded through NHS payments to LAs to support social care. A number of government policies have increased the scale of NHS payments to fund LA social care over time, including the Better Care Fund, which was introduced in FYE 2016 and aims to increase collaboration between NHS and LA bodies to support clients with long-term conditions.
Because the NHS is classified as central government in the national accounts, NHS expenditure is not included in the local government expenditure used to calculate the ASC inputs index, and so needs to be accounted for separately.
In the previously published ASC input measure, funding transfers from health services to LAs were incorporated in inputs by using data on central government expenditure on adult personal social services3 from the national accounts. However, as part of the review of the ASC productivity measure, these data have been replaced by data reported by LAs on income received from the NHS, as part of NHS Digital’s Adult Social Care Finance Return4, which provides a more detailed breakdown of NHS funding specifically for ASC5.
The NHS Digital Adult Social Care Finance Return analyses expenditure by source of funding, client type and service, more detail than is available for central government data in the national accounts. Use of this detailed data therefore enables a more holistic measure of adult social care expenditure, including NHS funding, to be used in the cost weights for output, more details of which can be found in Section 7.
However, it should also be noted that the Adult Social Care Finance Return only records data from LAs in England and so the change from national accounts data results in central government expenditure in the devolved administrations no longer being captured. In addition, the data series used are only available back to FYE 2005 and so there is a break in series between FYE 2004 and FYE 2005. This break in series is matched by changes in the output data described in Section 7.
The use of chain-linking growth rates to produce input and output indices means that although the expenditure coverage of the measure increases between FYE 2004 and FYE 2005, there is no step-change or “jump” in the input or output indices between these years.
Current price expenditure used in inputs
Figure 3 shows the expenditure used in ASC inputs in the previously published and new measures. The expenditure data are shown in current price terms, before deflation is used to convert the series into a quantity input series.
Figure 3: Current price expenditure series used in the calculation of adult social care inputs, previously published and new series
UK, 1997 to 2016
Source: Office for National Statistics
Notes:
- Current price expenditure for the new series has been converted to a calendar year basis to make it comparable with expenditure data used in the previously published series.
- Figures include Value Added Tax (VAT) and National Non-Domestic Rates (NNDR), paid by local authorities in the course of providing ASC. While LAs own accounts exclude the cost of these taxes as they are reimbursed by HMRC, VAT and NNDR are added back into expenditure data used in the national accounts in order to measure final consumption expenditure on a comparable basis with other sectors of the economy.
Download this chart Figure 3: Current price expenditure series used in the calculation of adult social care inputs, previously published and new series
Image .csv .xlsAs a result of the national accounts data for central government transfers to ASC being removed and the NHS Digital data on NHS funding for ASC not being available for the years before FYE 2005, the new expenditure data used in inputs is slightly less than in the previously published measure until 2004. For most of the period from 2004 onwards, the new measure of expenditure included in inputs is greater, though missing from the new measure is the increase in expenditure in 2012 – resulting from the inclusion of some housing services and social protection not elsewhere classified in the national accounts data used in the previously published series.
Deflating inputs
In addition to changes in expenditure, differences in inputs can also be attributed to the deflators used to remove the effect of inflation in input costs, to produce a quantity input measure.
ASC inputs are split into four main components, with separate deflators applied to each. Three of these components: the labour costs, LA intermediate consumption, and capital consumption, all relate to services provided directly by LAs and the fourth component is the expenditure on services commissioned by LAs from other providers. This fourth component primarily refers to services commissioned by LAs from independent sector providers, although the data used to determine the split between LAs’ own provision and other provision also include services commissioned by LAs from other LAs within the data for care provided by others. However, because independent sector provision makes up the great majority of care provided outside of LA own provision, and for ease of reading, the term independent sector provision is used in this publication to refer to care commissioned by LAs from providers other than themselves.
LA labour and capital consumption continue to be deflated by the same deflators that were used in the previously published ASC productivity measure.
The series used to deflate labour costs was developed by the Department of Health and Social Care. This measure uses workforce data from the Skills for Care National Minimum Data Set for Social Care to estimate the proportion of LA social care workers in different occupation groups, and uses data from the Annual Survey of Hours and Earnings to estimate changes in pay. Changes in the pay levels of different categories of ASC employees are weighted by the proportion of the total staff pay bill they account for, to calculate a deflator for the cost of labour.
Capital consumption is deflated by an implied deflator, which is not specific to ASC. While this is not ideal, it is the most suitable of the options currently available. However, as capital consumption represents a very small component of total ASC spending, the effect of using different capital deflators on the overall measure would be minor.
It should, however, be noted that the current measure of consumption of fixed capital for government services is due to be replaced with improved estimates for Blue Book 2019 and we intend to incorporate the new measure when available in a future public service productivity publication.
Changes to deflators
Changes have been made to the deflators used to produce the goods and services component of inputs, including both the intermediate consumption component of LAs’ own provision of ASC and LA purchases of care from the independent sector. Table 1 illustrates the changes made.
Table 1: Deflators used in previously published and new inputs series
| Inputs component | Deflator previous series | Deflator for new series | ||
|---|---|---|---|---|
| Local authority own provision | Labour | PSS Pay deflator | PSS Pay deflator | |
| Intermediate consumption | CPI | SAR-based intermediate consumption deflator | ||
| Capital consumption | Implied capital consumption deflator | Implied capital consumption deflator | ||
| Care provided by others | Direct payments | ISSCPI deflator | Direct payments deflator | |
| Other services | ISSCPI deflator | Independent sector labour/intermediate consumption deflator | ||
| Source: Office for National Statistics | ||||
| Notes: | ||||
| 1. PSS refers to personal social services, CPI refers to the Consumer Price Index, SAR refers to the Subjective Analysis Return and ISSCPI refers to the independent sector social care price index. | ||||
Download this table Table 1: Deflators used in previously published and new inputs series
.xls (28.7 kB)Intermediate consumption deflators for LA own-provided care
The intermediate consumption of LAs’ own provision of ASC has previously been deflated by the general Consumer Prices Index (CPI). However, this is not an ideal measure as the overall CPI measures the average price change of a household consumer’s basket of goods.
To better reflect the specific inflationary experience of social care services, new deflators have been matched to a more granular breakdown of expenditure. We have therefore constructed a basket of goods specific to LA social care using data from the Subjective Analysis Return (SAR), a data collection which records LA expenditure on different types of input for social care. These data are an extension of the subjective analysis in the Local Authority General Fund Revenue Account Outturn and are also used in Office for National Statistics (ONS) public service productivity statistics to produce input deflators for education and police services.
Different intermediate consumption items recorded in the SAR are deflated by suitable subcomponent indices of the CPI, Services Producer Price Index (SPPI), Producer Price Index (PPI) and Average Weekly Earnings (AWE, which is used in the case of agency staff). A composite deflator is then created by weighting each of these series together by the proportion of local authorities’ social care intermediate consumption expenditure they account for in the SAR6. The resulting “SAR deflator” is therefore more suitable than the overall CPI for producing the intermediate consumption input series.
Deflators for independent sector-provided care
LA purchases of care from the independent sector were previously deflated by an Independent Sector Social Care Prices Index (ISSCPI) provided by the Department of Health and Social Care. This deflator was built on the same ASC activity and spending data as used in the output measure. As a result, this method produced an implied deflator for the cost of independent sector-provided care to LAs.
However, as this deflator is a measure of the price inflation of independent sector-provided output, it is essentially an output deflator as opposed to an input deflator. Application of this deflator to expenditure on purchases of care from independent sector providers will therefore result in quantity input growth of a similar7 rate as quantity output growth. For example, if the data show an increase in weeks of care purchased from 1,000 to 1,100, both the output quantity and the input quantity of this component of the service would increase by 10% and productivity would not change. Therefore, the application of the ISSCPI deflator hinders measurement of the productivity of independent sector-provided care.
This is an issue as, since the start of our data series in 1997, the proportion of LA-funded ASC services provided by the independent sector has increased substantially and now accounts for the majority of ASC provision.
The coverage of ONS public service productivity measures is defined as services funded through public expenditure8 and is therefore not only limited to public sector providers, but also includes publicly-funded services provided by the independent sector. For the measure to be consistent with the Atkinson Review definition of public service and to remain relevant for users, productivity therefore needs to be measured for publicly-funded care purchased from the independent sector, in addition to public sector producers.
As a result, a method of deflation that is conceptually similar to that used for LA own-provision services, but using deflators specific to independent sector providers, has been applied to independent sector-provided services.
As with LA own-provided services, independent sector-provided ASC services will use labour and intermediate consumption inputs9. The ratio of expenditure made up of labour to intermediate consumption inputs is derived from FYE 2017 figures in LaingBuisson’s Care Cost Benchmarks report (PDF, 74.9KB) and FYE 2017 figures from the UK Home Care Association’s Minimum Price for Homecare estimates (PDF, 640.6KB), and this ratio is used to determine the proportion of independent sector inputs deflated by pay and intermediate consumption deflators.
The pay element accounts for approximately 68% of inputs and is deflated by a version of the Personal Social Services (PSS) pay index described earlier that is specific to the independent sector.
LaingBuisson’s Care Cost Benchmarks series and the UK Home Care Association’s Minimum Price for Homecare series also include analysis of the typical expenditure of independent sector providers on different goods and services inputs used in the provision of a week of residential and nursing care (in the case of Care Cost Benchmarks) or an hour of home care (in the case of Minimum Price for Homecare).
Using the same approach as the deflator for intermediate consumption for LA-provided services, a basket of goods has been created from these two publications and each element deflated by an appropriate CPI, SPPI or PPI deflator to create a deflator for independent sector intermediate consumption. The relative weights given to the Care Cost Benchmarks and Minimum Price for Homecare data in the deflator are determined by the relative expenditure on residential and nursing care and home care reported in the data from NHS Digital.
Expenditure on direct payments is deflated separately and the deflated direct payments data are used in both inputs and output. More detail on the deflator used for direct payments can be found in Section 7.
Figure 4 shows how different deflator series have changed over time.
Figure 4: Indices for deflators used in previously published and new adult social care inputs series
UK, financial year ending 1997 to financial year ending 2017
Source: Office for National Statistics
Download this chart Figure 4: Indices for deflators used in previously published and new adult social care inputs series
Image .csv .xlsInput deflators reflect the cost pressures faced by service providers. Higher deflator growth results in lower input growth, as higher costs mean any given level of expenditure purchases fewer inputs.
Over the course of the series, inflation faced by social care providers has been greater than the general price inflation faced by households, as measured by the CPI, although for certain periods this difference has been reversed. In particular, the specific deflators for ASC intermediate consumption have experienced inflation lower than CPI for most of the period since FYE 2011.
Figure 4 shows only small differences between the specific ASC intermediate consumption deflators, with the home care deflator experiencing slightly more volatility, due partly to the relatively high weight of travel costs in the home care deflator.
Labour deflators, which affect the overall input measure more than intermediate consumption due to the greater spending share of labour, have also experienced greater growth than the overall CPI over the whole series, partly reflecting higher real-terms wages in the social care sector in FYE 2017 than in FYE 1997.
Over the series the labour deflators have also grown faster than the intermediate consumption deflators and as with the intermediate consumption deflators, there are minimal differences between LA and independent sector input inflation.
However, the labour deflators grew more slowly than the intermediate consumption deflators between FYE 2007 and FYE 2014, a period characterised by lower wage growth in the general economy. Inflation in labour costs exceeded inflation in intermediate consumption costs again after FYE 2014 and the labour deflators grew particularly quickly in FYE 2017, partly due to the introduction of the National Living Wage. As many social care jobs are paid at or near the National Living Wage, its introduction has resulted in a significant cost pressure for social care providers10.
Over the whole 20-year series, the switch from CPI to the SAR-based deflator results in lower growth in inputs for LA intermediate consumption in the new measure relative to the previously published measure, while the switch from the ISSCPI to the combined independent sector input deflator results in higher growth for independent sector inputs in the new measure.
A separate deflator is applied to direct payments and more information on this can be found in Section 7.
Effect of changes on inputs
Figure 5 shows a comparison of the inputs measure included in the previously published ASC productivity series and the measure used in the new series.
Figure 5: Public service adult social care inputs indices, new series and previously published series
UK, 1997 to 2016
Source: Office for National Statistics
Download this chart Figure 5: Public service adult social care inputs indices, new series and previously published series
Image .csv .xlsThe introduction of NHS funding in the expenditure measure has had an upward effect on inputs growth for the years after it was included in FYE 2005, as NHS funding has grown more quickly than other LA spending. In addition, for most years of the series, changes in the deflator series used have also resulted in faster inputs growth.
However, the new series does not experience the same inputs growth as the previously published series in 2012, due to the removal of housing and social protection not elsewhere classified expenditure, which had previously been included in the adult social care series from 2012 onwards.
Figure 6 shows the contribution to overall ASC inputs growth from each of the three components that inputs can be divided into.
Figure 6: Contributions to inputs growth by labour, goods and services, and capital consumption
UK, financial year ending 1998 to financial year ending 2017
Source: Office for National Statistics
Notes:
- Data are displayed on a financial year basis prior to conversion to calendar year. Growth rates refer to the contribution to overall input growth between the stated year and the previous year. For example, the figures for FYE 2015 refers to the contributions to input growth between FYE 2014 and FYE 2015.
Download this chart Figure 6: Contributions to inputs growth by labour, goods and services, and capital consumption
Image .csv .xlsFigure 6 shows almost all growth over the period has been driven by goods and services, due primarily to increases in the procurement of care from independent sector providers, which are entirely recorded in the goods and services component of inputs.
Notes for: Measuring inputs
Inputs for Scotland use budgeted as opposed to outturn expenditure data for financial year ending 2017 as outturn expenditure data are not yet available.
Also known as consumption of fixed capital, capital consumption covers the cost of depreciation of capital goods (items that are anticipated to be in use over several years and add to the stock of resources in the ASC system, such as buildings) over time.
The coverage of adult personal social services matches the coverage of adult social care, but the different terminology is used within the Classification of the Functions of Government system in the national accounts.
Data from the Personal Social Services Expenditure and Unit Costs Return, which preceded the Adult Social Care Finance Return were used for the years before FYE 2015.
Included in expenditure on both the input and output side are the NHS Digital lines for NHS income, income from joint arrangements and other income. This approach mirrors the approach taken by NHS Digital as part of their ASC unit costs analysis. It should be noted that the other income line also includes transfers between LAs to fund clients who are provided a care placement in another LA to their own. The NHS Digital data collection is set up such that each LA should record expenditure and activity data only for clients whose care they are responsible for, meaning expenditure and activity on each client receiving care from a different LA to the one responsible for funding them should only be recorded once. However, in some cases, LAs are unable to separate their own expenditure from expenditure by other LAs, resulting in some probable double counting, although the scale of this double counting is not known. More discussion of NHS transfers to LAs can be found in NHS Digital’s Adult Social Care Activity and Finance Report, England 2016-17.
The basket of goods derived from the SAR used to produce the LA intermediate consumption is modified from the original SAR basket to remove procurement of care from the independent sector, as the intermediate consumption of independent sector providers is deflated separately.
Due to small differences in the calculation of output via a cost-weighted activity index and via the application of an output deflator, the rate of volume growth for inputs and output will not be identical where multiple different types of activity are being combined into an index.
Public service productivity statistics are based on a concept of output as measured by government consumption expenditure rather than government production. This means that we are using a measure of government-purchased output, regardless of what type of business unit produced the output. As with other aspects of the methodology employed in producing these statistics, this approach is consistent with that recommended by the Atkinson Review (PDF, 1.08MB). The adult social care productivity measure therefore includes output produced by business units that are classified as private businesses or non-profit institutions serving households (NPISH) in the UK National Accounts, and this is why the term “public service” is used instead of “public sector”.
Capital consumption has not been deflated separately for independent sector-provision. This is because no separately identified estimates for independent sector ASC capital consumption are available on a consistent basis to the capital consumption estimates in the national accounts. In addition, the deflators for capital consumption that are available in the national accounts are not specific to individual public service sectors. However, given the small element of capital in LA own-provision ASC, exclusion of specific deflators for independent sector capital consumption should not make a major difference to the measure.
Further information on the cost pressures on social care providers from the National Living Wage is available in the ADASS Budget Survey (PDF, 1.2MB).
7. Measuring quantity output
There are a number of developments to the measure for adult social care (ASC) output in England including:
introduction of a new cost-weighted activity index for the new data source for England from financial year ending 2015 (FYE 2015) onwards
improvements to the cost-weighting of activity for the years before FYE 2015, including the incorporation of NHS spending and merging the cost weights for local authority (LA) and independent sector provided residential care
modification of activity data to better align with inputs and NHS Digital’s unit costs analysis
incorporation of “output-equals-inputs” elements of output, for services where data on the number of activities carried out is not available, including direct payments
use of “output-equals-inputs” estimation for the output growth rate between FYE 2014 and FYE 2015
Measuring output: cost-weighted activity
Where data on the number of activities undertaken in a public service are available, quantity output (also known as volume output) is measured using a cost-weighted activity index. This index is produced by calculating the growth rates of different ASC activities and weighting these by their unit costs. As a result, growth in activities that are high-volume and expensive has a greater effect on the output index than a similar rate of growth in activities that are uncommon and low-cost.
For England, data for this measure are taken from NHS Digital, which collects the data from English LAs, and for Scotland data are provided by the Scottish Government. Activity data for Wales and Northern Ireland are not available and so output in these nations is assumed to grow at the same rate as the rest of the UK. The methodology for ASC output for Scotland has not changed in this publication, although output for Scotland is forecast for FYE 2017 as these data are not yet available.
Because the measures in this analysis are for public service output and productivity, activity data are scaled down to net off the proportion of service funding that comes from client contributions, and to ensure that the output measure aligns with the inputs by only including publicly-funded ASC activity.
Output measured through a cost-weighted activity index is also known as directly-measured output, in contrast to output measured through the “output-equals-inputs” approach, which is known as indirectly-measured output.
Changes to output data source
Following a Zero Based Review, NHS Digital (formerly the Health and Social Care Information Centre) implemented changes to the data they collect from LAs in England on ASC.
While aggregated expenditure remained consistent, breakdowns by client and service types are not comparable between the pre-review and post-review collections. As cost-weighted activity could no longer be measured on a comparable basis from financial year ending 2014 (FYE 2014) onwards, ASC output was forecasted for the period following the implementation of the Zero Based Review in the last two editions of Public service productivity estimates: total public service.
The range of services for which activity data are collected in the post-review NHS Digital data collection is substantially reduced relative to the pre-review collection, although it still includes residential and nursing care, which are among the largest services in terms of expenditure. Table 2 details the services for which activity data are available from the two collections, ordered by the proportion of expenditure they account for in the latest year used.
Table 2: Services in England for which output is measured using activity data, financial year ending 2013 and financial year ending 2016
| Percentage | |||||||
|---|---|---|---|---|---|---|---|
| NHS Digital pre-review data collection (until FYE 2014) | Proportion of expenditure (FYE 2013) | NHS Digital post-review data collection (from FYE 2015 onwards) | Proportion of expenditure (FYE 2016) | ||||
| Residential care | 29.7 | Residential care | 25.0 | ||||
| Home care | 17.0 | Nursing care | 7.4 | ||||
| Referrals and assessments | 12.7 | Short-term care to maximise independence | 3.3 | ||||
| Nursing care | 7.7 | ||||||
| Day care | 7.0 | ||||||
| Equipment and adaptations | 2.0 | ||||||
| Meals | 0.2 | ||||||
| Output for other services measured indirectly using “output-equals-inputs” approach | 23.8 | Output for other services measured indirectly using “output-equals-inputs” approach | 64.3 | ||||
| Source: Office for National Statistics | |||||||
| Notes: | |||||||
| 1. As the output index is produced using a Laspeyres approach, previous-year cost weights are used to weight together the activity growth of different components. Figures are therefore given for financial year ending (FYE) 2013 and FYE 2016, as these are the final cost-weights used from the pre-review data and the most recent cost-weights used in the post-review data. | |||||||
Download this table Table 2: Services in England for which output is measured using activity data, financial year ending 2013 and financial year ending 2016
.xls (29.7 kB)Residential and nursing care activity are further split by client type in both pre- and post-review data collections1, and referrals and assessments, and day care were split by client type in the pre-review data. The data collection used to calculate ASC output in Scotland is unaffected by these changes. Activity data for Scotland cover residential and nursing care, home care and day care, all split by client type, and the number of meals provided.
Incorporation of NHS-funded activity
In the previously published output series, the activity data used excluded clients in LA-arranged residential and nursing care who were fully funded by the NHS2. As the new measure incorporates NHS expenditure in the inputs, the residential and nursing care activity data have also been changed to include clients in LA-arranged care fully funded by the NHS in the output.
Changes to cost-weights
Cost weights are used to determine the relative size of effect different types of activity have on output. More expensive forms of output are assumed to have a greater value and so an increase of one unit of activity has a greater effect on output where that activity has a higher cost-weight.
The previously published ASC output measure used LA net current expenditure by service and client type to derive unit costs for each different unit of activity.
To be consistent with the inputs and the activity data, the new measure incorporates NHS funding into the cost weights using the same NHS Digital data used in the inputs.
Further changes have been made to the cost weights to include capital charges, which reflect capital consumption, a relevant part of the total cost of providing services, and to exclude grants given to voluntary organisations, as the activity these grants fund is not covered in the activity data we use.
These changes also affect the calculation used to net down activity data for client contributions.
Using merged cost weights for LA-provided and independent sector-provided residential care
In both the previously published output series and the new output series, cost weighting is carried out using unit costs assigned for different services types and different client types. For instance, separate cost weights will be allocated to a week of nursing care for older people and to a week of nursing care for adults aged under 65 years with a physical disability, reflecting the differing cost of providing care to these different client groups.
In the previously published series, separate cost weights were also allocated in the England data to weeks in residential care for different client types depending on whether they were provided by LAs or independent sector providers3. NHS Digital’s unit cost analysis demonstrates the differences between the two provider types, with unit costs for residential care for older people over 50% higher in LA-provided care and unit costs for care for younger adults with learning disabilities around 25% to 50% higher.
In the previously published output series, these unit cost differences were reflected in the cost weights assigned to LA-provided and independent sector-provided residential care. The higher cost weights for LA-provided care meant changes in the number of weeks provided by LAs had a greater effect on the output index than changes in the number of weeks provided in the independent sector.
Since the mid-2000s, the number of weeks in residential care provided by LAs has fallen at a considerably faster rate than the number of weeks provided by the independent sector. As a result of the higher cost weights for LA-provided care in the previously published series, the effect of residential care on reducing ASC output was more than proportional to the fall in the total number of weeks provided over the period.
Differences in unit costs between LA and independent sector provision may be due to a range of factors, with some of the possible reasons relating to input costs and efficiency. LaingBuisson’s Care of older people: UK market report (PDF, 538.7KB) suggests the difference between LA-provided and independent sector-provided care may be due partly to higher costs from more generous employment terms and conditions in the LA sector. In addition, LaingBuisson report that LAs can secure lower prices for residential care from independent sector providers than private clients can, by procuring multiple care home places from providers4. This may also lower the unit costs of residential care purchased by LAs from independent sector providers relative to LA-provided care.
Differences may also be due to the nature of the service provided. LaingBuisson also suggest differences may be due to LA providers focusing on more short-term forms of care such as respite and intermediate care, or due to differences in the quality of care provided. However, for the years following NHS Digital’s Zero Based Review in FYE 2015, any effect of higher unit costs for shorter-term care in LA provision should be reduced as short-term care activity is recorded separately to other residential care, while the new quality adjustment (explained in Section 8) should capture changes in the quality of care over time.
Following these developments, a method change has been implemented so that the new ASC output index uses the same weight for each week in residential care provided by LAs and independent sector providers. Different cost weights continue to be used for different client types, reflecting the variation in the intensity of care needed by different client groups.
Figure 7 shows that implementation of this methods change results in greater output growth across the period, although the effect of the change in any given year is relatively small.
Figure 7: Public service adult social care non-quality adjusted output indices with alternative treatments for residential care cost weights
UK, 1997 to 2016
Source: Office for National Statistics
Download this chart Figure 7: Public service adult social care non-quality adjusted output indices with alternative treatments for residential care cost weights
Image .csv .xlsIncorporation of “output-equals-inputs” services
Previously, ASC output has been measured only for services where activity data are available, a form of output known as directly-measured output. However, as a result of the new data collection, the range of services for which activity data are available is substantially reduced.
To mitigate against this loss of output data, ASC services for which activity data are not available are included in the output measure on an “output-equals-inputs” basis, also known as indirectly-measured output. This means that output is estimated to grow at the same rate as input for services without activity data. As a result, productivity growth for these services is assumed to be zero.
This treatment ensures the productivity measure is not affected by differences between output and input growth caused by a mismatch between the coverage of services included in inputs and the coverage of services included in output. However, inclusion of services through the “output-equals-inputs” method has a dampening effect on productivity, reducing the scale of productivity changes. To view the productivity trend without this dampening effect, Section 11 includes an alternative series measuring changes in productivity for services with directly-measured output only, on an England financial year basis.
Due to data limitations, the “output-equals-inputs” method is only applied to data from England.
Direct payments
Direct payments involve LAs providing funding to care clients to enable them to arrange and pay for the care themselves, in place of the LA commissioning the care for them.
As with other indirectly-measured services, output and input for direct payments are measured by deflating expenditure with the most appropriate deflators available.
To produce a deflator for direct payments, we conducted a small survey of LAs with the assistance of the London Association of Directors of Adult Social Services (ADASS) Improvement Programme, receiving responses from six councils. The results of the survey suggested that approximately 46% of direct payments spending was on home care, 35% on other care services (including day and respite care) and 19% was on other goods and services (including transport). Using these figures as weights, a composite deflator was constructed from the Consumer Prices Index (CPI) subcomponents of home care and social protection, with general CPI used to deflate other goods and services.
As direct payments are included on an “output-equals-inputs” basis, direct payments expenditure is also deflated by the same deflator in the inputs as in the output, resulting in zero productivity growth.
Although direct payments have been included in the ASC output and input measures in this publication to reflect changes in the nature of ASC provision, direct payments are not currently classified within public sector output in the national accounts, as they are classified as a transfer payment from government to households. When the new ASC output series are incorporated in the national accounts output, the current treatment of direct payments will be subject to further review.
Estimation of output growth between FYE 2014 and FYE 2015
As a result of the change in the NHS Digital data collection between FYE 2014 and FYE 2015, it is not possible to measure changes activity on a consistent basis between FYE 2014 and FYE 2015. As a result, no direct measures of output using activity data are used to calculate the growth rate between these two years. Instead, total ASC output was estimated on an “output-equals-inputs” basis for England using total ASC expenditure and a composite deflator constructed from all deflators used for ASC inputs.
Figure 8: Change in non-quality adjusted output, previously published and new series
UK, 2013, 2014 and 2015
Source: Office for National Statistics
Download this chart Figure 8: Change in non-quality adjusted output, previously published and new series
Image .csv .xlsThe impact of the bridging year is illustrated in Figure 8, which shows that the implementation of the “output-equals-inputs” approach for England resulted in a slightly greater fall in output in 2014 than the previous year, but the output fall in 2014 is reduced relative to the predominantly forecast estimate in the previously published series.
Effect of changes on output
Figure 9 shows the new non-quality adjusted output measure in comparison with the previously published output series.
Figure 9: Public service adult social care output indices, new non-quality adjusted series and previously published series
UK, 1997 to 2016
Source: Office for National Statistics
Download this chart Figure 9: Public service adult social care output indices, new non-quality adjusted series and previously published series
Image .csv .xlsFigure 9 shows that the new series experiences stronger growth than the previously published series, particularly after 2002, when the “output-equals-inputs” component grows following the introduction of spending from the Supporting People scheme into adult social care, and the expansion of direct payments and other “output-equals-inputs” services, such as supported accommodation.
Notes for: Measuring quantity output
More data on adult social care activity can be found in NHS Digital’s Adult Social Care Activity and Finance Report.
Clients fully funded by the NHS cover those funded under Section 256 of the NHS Act 2006. As with the choice of NHS funding data included in the inputs, the change to include these clients mirrors the approach taken by NHS Digital in their unit costs analysis.
As with inputs, the data used to determine the split between LA provision and other provision include services commissioned by LAs from other LAs within the data for care provided by others. However, because independent sector provision makes up the great majority of care provided outside of an LA’s own provision, and for ease of reading, the term independent sector provision is used to refer to care commissioned by LAs from providers other than themselves.
More information on local authority procurement of residential care is available from the House of Commons Library – Social care: care home market briefing paper (PDF, 186KB).
8. Quality adjustment
This publication also introduces a new quality adjustment for adult social care (ASC) output.
Quality adjustments to public service output were a recommendation of the Atkinson Review on the measurement of government output and productivity for the national accounts (PDF, 1.1MB), which stated: “The output of the government sector should in principle be measured in a way that is adjusted for quality, taking account of the attributable incremental contribution of the service to the outcome.”
Quality adjustments are applied to output to counter the limitations of using cost weights to value different types of activity in quantity output measures. For instance, while quantity output may be growing, the value of this growth, and therefore productivity, may be overstated if service quality is declining.
The ASC quality adjustment introduced here uses the concept of adjusted social care-related quality of life, which is established within the Adult Social Care Outcomes Framework (ASCOF), and data from the Adult Social Care Survey in England.
As no equivalent data source measuring care-related quality of life is available for the devolved administrations, the quality adjustment for ASC is applied to UK output, under the equivalent convention to current quality adjustments in other public service productivity sectors1.
The following section introduces the methodology for this adjustment and analyses its effect.
Data source and framework for quality adjustment
The Adult Social Care Survey (ASCS) is a sample survey of clients in local authority (LA)-supported care2 in England conducted from financial year ending 2011 (FYE 2011) onwards. The survey’s sample coverage includes clients whose care is partly- or wholly-funded by a LA, including those in receipt of direct payments, or clients in LA-organised care who are fully self-funding.
In FYE 2017, the survey interviewed around 73,000 clients out of a total eligible population of around 656,000 clients, with data from 58,000 respondents sufficiently detailed to be used in our quality adjustment.
Data collected by the ASCS include clients’ age, gender, type of care and funding, self-reported health status, activities that clients need support with, and the degree to which their needs are met.
Results from the ASCS are used to produce a range of service performance measures, which are published in the Adult Social Care Outcomes Framework (ASCOF)3.
The objective of quality adjustment is to adjust output for the value of the service being provided. Therefore, an ideal quality adjustment reflects the degree to which a service improves outcomes for service users. For adult social care services, a critical outcome is the improvement of clients’ quality of life, relative to how it would be in the absence of care services.
Two of the measures within the ASCOF specifically measure clients’ quality of life. “Measure 1A”, defined as social care-related quality of life, is calculated from clients’ responses to how well their needs are met (on a scale from “no needs met” to “no unmet needs”) across eight domains:
control
personal care
food and nutrition
accommodation
safety
social participation
occupation
dignity
“Measure 1J”, defined as adjusted social care-related quality of life, builds on the concept of “measure 1A” to derive a measure that isolates the impact of ASC services’ performance on quality of life.
This involves two main changes relative to “measure 1A”. Firstly, each level of response on care needs across each of the eight domains is weighted to account for its importance in affecting quality of life, using weights developed from a separate survey of community care users4. Secondly, factors predominantly outside the influence of ASC services, but which affect the likelihood of needs being met, are controlled for. These factors include clients’ age, health status, suitability of clients’ home for meeting their needs and clients’ ease of travelling around outside in their local environment.
The quality adjustment used for output and productivity is produced using the concept of ASCOF “measure 1J”, although separate methods are implemented for community care services and residential and nursing care services.
Quality adjustment for community care
While NHS Digital have published the “measure 1J” only for FYE 2017, data from the ASC Survey itself are available from FYE 2011 onwards. In addition, the “measure 1J” is not published for different client types and does not include clients with learning disabilities.
To produce the quality adjustment for community care, we implemented the calculation of “measure 1J” on the ASC Survey. The figures produced for the quality adjustment will differ slightly from the published ASCOF figures but this approach has several advantages for use in a quality adjustment. Firstly, it enables the production of a time series from the start of the ASC Survey in FYE 2011.
Secondly, it enables the quality adjustment to be extended to learning disability clients, who make up a substantial proportion of service output weighted by spending. While the study used to derive the weights for the eight domains of care-related quality of life included a small subsample of learning disability clients, the results of this study have not been applied to the published “measure 1J” pending further work. However, learning disability clients continue to be covered by the ASC Survey and a separate “easy-read” questionnaire is provided for respondents with learning disabilities. To ensure the quality adjustment includes all client types, adjusted social care-related quality of life is estimated for learning disability clients using the same preference weights for the eight domains of quality of life as are used for other clients.
Thirdly, calculation of “measure 1J” from the ASC Survey enables the production of separate quality adjustments for different client types, with separate adjustments produced for older adults, younger adults with learning disabilities, who are identified through use of the “easy-read” questionnaire5, and younger adults with other needs. This improves the overall quality adjustment as the quality adjustments for each client type are specifically applied to the associated output for each client type. The separate quality adjustments also improve the precision of the productivity measures for the analysis by service type and client type in Section 11.
The quality adjustments for each individual in the ASC Survey dataset are weighted to account for variation in survey completion rates by local authority. The quality adjustment for community care is then calculated as the change in adjusted social care-related quality of life from one year to the next.
Quality adjustment for residential and nursing care
Because the weights for the domains of quality of life in “measure 1J” are produced using a survey of community care users and the adjustment applied to account for items outside the control of ASC services is specific to community care, a separate approach is taken to quality adjust residential and nursing care output.
The residential and nursing care quality adjustment draws on work conducted by Yang, Forder and Nizalova (2017) at the Personal Social Services Research Unit for analysing residential and nursing care quality by region.
This quality adjustment uses a regression-based approach to measure the strength of association with care-related quality of life of a range of factors that are outside ASC providers’ control, and so need to be controlled for to derive the change in quality of life attributable to the performance of ASC services. The factors used in the regression model are:
gender
ethnicity
age
self-reported health status, level of pain and level of anxiety
the number of basic activities of daily living (ADLs) the client needs support with
whether the client can deal with their finances and paperwork
The quality adjustment is calculated as the change in average social care-related quality of life minus the change in expected average social care-related quality of life based on the regression model. This ensures that, for instance, if care-related quality of life is shown as increasing, the change used in the quality adjustment only incorporates the change in care-related quality of life attributable to ASC services.
For most of the years for which the quality adjustment was calculated, the quality adjustment grew more slowly than care-related quality of life, as a result in improvements in expected quality of life, due mainly to a fall in the proportion of clients reporting bad health and a rise in the proportion of clients reporting good health.
As with the community care adjustment, the adjustment for residential and nursing care is carried out separately for older adults, younger adults with learning disabilities (as identified by the “easy-read” questionnaire) and younger adults with other needs.
Results of quality adjustment
Table 3 shows changes observed in each of the six elements of the quality adjustment. This suggests that quality improvements were generally greater for community care than residential care over the series, but caution should be taken in interpreting this difference, due to differences in the methodology used.
No quality adjustment was measured for growth between FYE 2014 and FYE 2015, as a change in client eligibility for the ASC Survey resulted in a break in series between these two years6.
Table 3: Percentage change in components of adult social care quality adjustment, financial year ending 2011 to financial year ending 2017
| Percentage change | |||||||
|---|---|---|---|---|---|---|---|
| 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | ||
| Residential and nursing care – older adults | 1.2 | 0.2 | -1.3 | 0.0 | -0.5 | 1.0 | |
| Residential and nursing care – younger adults with learning disabilities | 0.1 | -0.2 | 0.0 | 0.0 | 2.1 | -0.4 | |
| Residential and nursing care – younger adults with other needs | -0.3 | 0.3 | 0.8 | 0.0 | 2.1 | -1.3 | |
| Community based care – older adults | 2.4 | 1.4 | 1.4 | 0.0 | 0.5 | 1.2 | |
| Community based care – younger adults with learning disabilities | 6.4 | -0.7 | 1.7 | 0.0 | 0.1 | -0.2 | |
| Community based care – younger adults with other needs | 2.7 | 0.1 | 2.1 | 0.0 | 0.7 | 3.4 | |
| Source: Office for National Statistics | |||||||
| Notes: | |||||||
| 1. Growth rates for each year are given as the growth between the stated year and previous year. For example, the growth figure for FYE 2017 is the growth measured between FYE 2016 and FYE 2017. | |||||||
Download this table Table 3: Percentage change in components of adult social care quality adjustment, financial year ending 2011 to financial year ending 2017
.xls (28.7 kB)Figure 10 shows the effect of the quality adjustment on output. Because the quality adjustment is produced from financial year data, a process known as “cubic splining” is used to convert the data to a calendar year basis for application to the output measure. The cubic splining process also backcasts the quality adjustment by one quarter to obtain a growth rate between calendar years 2010 and 2011.
Figure 10: Quality adjusted and non-quality adjusted output indices
UK, 2010 to 2016
Source: Office for National Statistics
Download this chart Figure 10: Quality adjusted and non-quality adjusted output indices
Image .csv .xlsFigure 10 shows that the quality adjustment increased output most in 2011, the first year it was applied. Overall, the quality adjustment increases output by 5.1% relative to its non-quality adjusted level in 2016.
As ASCOF “measure 1J” was only published in FYE 2017, “measure 1A” is the most relevant published ASCOF series for measuring quality change over time. As with the quality adjustment, “measure 1A” showed improvements between FYE 2011 and FYE 2014, though there was no further improvement in “measure 1A” at the one decimal point level after the change in sample from FYE 2015, when lower quality growth was also observed for the output quality adjustment.
Section 9 analyses the effect of the quality adjustment on productivity.
Notes for: Quality adjustment
It should be noted that we intend to review the current approach to the geographical application of quality adjustment across all quality adjusted sectors and future changes could result in quality adjustments only being applied to output from the same constituent nations as the quality adjustment data is obtained from.
LA-supported care refers to care that is partly or wholly funded by LAs or care provided by LAs.
Further information on how measures within ASCOF are constructed can be found in the ASCOF Handbook of Definitions (PDF, 1.4MB).
For more information on how “measure 1J” is produced and the study used to derive the weights for the eight domains, see Identifying the impact of adult social care (IIASC).
It should be noted that not all clients with learning disabilities will have completed the “easy-read” questionnaire and not all clients aged under 65 years who complete the “easy-read” questionnaire will necessarily have learning disabilities. However, in the large majority of cases, use of the “easy-read” questionnaire should separate the learning disability and non-learning disability clients in the younger age group.
The main changes to sample coverage of the ASC Survey made for the FYE 2015 data onwards were to remove clients receiving low-level support only and include clients paying the full cost of care themselves. More detail on these changes can be found in the NHS Digital publication, Adult Social Care Survey, England – 2014-15.
9. Analysis of the new adult social care productivity series
Public service productivity is estimated by comparing growth in the total quantity of output provided with growth in the total quantity of inputs used. Figure 11 shows adult social care (ASC) inputs, non-quality adjusted output and non-quality adjusted productivity. It should be noted that while most data have been updated to 2016, data for Scotland are not yet available for the final year of the series and so ASC output for Scotland is forecast and ASC inputs use budgeted as opposed to outturn expenditure for Scotland for this final year.
Figure 11: Public service adult social care non-quality adjusted output, inputs and productivity indices
UK, 1997 to 2016
Source: Office for National Statistics
Download this chart Figure 11: Public service adult social care non-quality adjusted output, inputs and productivity indices
Image .csv .xlsFigure 11 shows the new ASC non-quality adjusted productivity measure fell over the series by an average rate of 0.9% per year.
Volumes of inputs and non-quality adjusted output grew quickly between 1997 and 2005 at an average rate of 4.5% and 3.5% respectively. Since 2005, these two series have experienced smaller changes, with inputs 5.7% higher in 2016 than 2005 and non-quality adjusted output 4.6% lower.
Figure 12 shows how the new non-quality adjusted measure of productivity compares with the previously published productivity measure, which was also non-quality adjusted.
Figure 12: Public service adult social care productivity; comparison between new non-quality adjusted productivity and previously published measure
UK, 1997 to 2016
Source: Office for National Statistics
Download this chart Figure 12: Public service adult social care productivity; comparison between new non-quality adjusted productivity and previously published measure
Image .csv .xlsThe new, non-quality adjusted productivity measure experiences less of a fall than the previously published series, which declined by 27.3% in total between 1997 and 2015. This is in contrast with the new series, which fell by 17.0% over the same period.
It is notable that the new measure does not experience as large a fall in productivity in 2012, which was present in the 2018 edition of total public service productivity as a result of the reclassification of housing services expenditure in the national accounts. The reversal of this reclassification results in a smaller fall in productivity in 2012 in the new series.
Figure 13 shows the effect of the incorporation of the quality adjustment on productivity.
Figure 13: Public service adult social care productivity; comparison between quality adjusted and non-quality adjusted productivity
UK, 1997 to 2016
Source: Office for National Statistics
Download this chart Figure 13: Public service adult social care productivity; comparison between quality adjusted and non-quality adjusted productivity
Image .csv .xlsBoth the quality adjusted and non-quality adjusted measures of productivity fell in 2012, but productivity performance improved after 2012. The quality adjustment had a positive effect on productivity for the years it was present, adding 0.8% to productivity growth on average between 2010 and 2016. Quality adjusted productivity was 2.6% lower in 2016 than 2010 in contrast with non-quality adjusted productivity, which was 7.4% lower.
Nôl i'r tabl cynnwys10. Adult social care productivity for England on financial year basis
Public service adult social care (ASC) productivity statistics have previously been produced for the UK only and on a calendar year basis, an equivalent geography and periodicity to UK National Accounts products, such as the Blue Book, which share much of the data. In this section, we include the inputs, output and productivity series for England on a financial year basis (that is, 1 April to 31 March).
These figures have been produced to provide a measure to ASC policy analysts, which is on a more consistent basis with other statistics that cover the English adult social care sector, including client numbers and measures of client need, which are analysed later in this section. The changes that have been made to data sources and methodology to produce an England financial year estimate, also enable the production of several new productivity measures, including for different types of care and different client age groups.
However, it should be noted that as a result of these changes and differences in the coverage of output and input measures across the UK, differences between the UK and England productivity measures cannot be used to estimate productivity growth in the devolved administrations1.
Differences between England financial year and UK calendar year productivity
In addition to only using data from England, the England financial year productivity measure takes expenditure data from NHS Digital’s Adult Social Care Activity and Finance Return (and its predecessors), in contrast with the UK calendar year measure, which is mainly produced using local authority data from the national accounts. This change is made as the NHS Digital data enable the analysis of productivity by service and client type.
The difference in data sources results in a further difference between the England and UK input measures, as the local authority expenditure data from NHS Digital used in the England measure are not adjusted for Value Added Tax (VAT) and National Non-Domestic Rates (NNDR). VAT and NNDR are added to local authority expenditure in the national accounts (and therefore UK inputs) for calculating final consumption expenditure2.
Furthermore, the “cubic splining” process used to convert financial year data to calendar year is not carried out in the production of the England financial year measure.
The combination of differences in data sources, treatment of VAT and NNDR, geographical coverage and the use of cubic splining in the UK but not the England measure mean that year-on-year growth rates of the UK calendar year inputs and England financial year inputs may differ substantially.
Several data sources are shared between the UK and England productivity measures, including the capital consumption measure, the deflator series and the spending data used to apportion input spending to different deflators. The quality adjustment, which is produced using data for clients in England only, remains the same in the England financial year measure.
Analysis of productivity on an England financial year basis
Figure 14a shows the inputs, output and productivity series for England on a financial year basis over the whole series, while Figure 14b focuses on the period after the introduction of the quality adjustment in financial year ending (FYE) 2011. Despite differences between the England and UK measures in the data sources for ASC expenditure and activity in the UK, the productivity trend for the England financial year measure is similar to that for the UK calendar year measure.
Figure 14a: Public service adult social care inputs, output and productivity indices, quality adjusted and non-quality adjusted
England, financial year ending 1997 to financial year ending 2017
Source: Office for National Statistics
Download this chart Figure 14a: Public service adult social care inputs, output and productivity indices, quality adjusted and non-quality adjusted
Image .csv .xls
Figure 14b: Public service adult social care inputs, output and productivity indices, quality adjusted and non-quality adjusted
England, financial year ending 2011 to financial year ending 2017
Source: Office for National Statistics
Download this chart Figure 14b: Public service adult social care inputs, output and productivity indices, quality adjusted and non-quality adjusted
Image .csv .xlsFigure 14a shows ASC productivity in England falling between financial year ending 1997 (FYE 1997) and financial year ending 2011 (FYE 2011), the year prior to the introduction of the quality adjustment, at an average rate of 1.0% per year.
For the period after FYE 2011, as shown by Figure 14b, non-quality adjusted ASC productivity has fallen further, but at a reduced rate of 0.4% per year. The positive quality adjustment from the years FYE 2011 onwards results in quality adjusted productivity growing over this period, at an average rate of 0.4% per year.
Inputs and output have increased in the last two years of the series. This may be due partly to the Better Care Fund, a funding transfer from the NHS to local authorities introduced in FYE 2016, which aims to improve efficiency and outcomes across health and social care by facilitating closer co-ordination between the two services. While both inputs and output have increased slightly following the introduction of the Better Care Fund, non-quality adjusted productivity fell marginally, while quality adjusted productivity rose marginally.
Comparison with a crude productivity indicator using client numbers
NHS Digital also publish statistics on the number of clients receiving social care in England. Figure 15 combines an index of the number of clients receiving care with an index of total ASC spending in England deflated by a general gross domestic product (GDP) implied deflator to produce a cruder productivity measure than that introduced in this article. This cruder productivity measure shows a greater decline in productivity than the new public service productivity measure, with a greater fall in crude “output” and a greater rise in crude “input”, although it should be noted that the client numbers series has a major break in series between FYE 2014 and FYE 2015.
Figure 15: Comparison of public service adult social care productivity indices compared with crude input, output and productivity indicators
England, financial year ending 2005 to financial year ending 2017
Source: Office for National Statistics
Notes:
- There is a break in series in the number of clients receiving long-term support at year-end between FYE 2014 and FYE 2015 due to a change in data source. Prior to FYE 2014, this measure is the sum of clients in receipt of LA community or residential or nursing care at year-end.
Download this chart Figure 15: Comparison of public service adult social care productivity indices compared with crude input, output and productivity indicators
Image .csv .xlsThese data show a steady decline in the number of clients receiving care in England, in contrast with the output measure included in this article. Research by the Centre for Analysis of Social Exclusion (CASE) at the London School of Economics (LSE) suggests this may be as a result of the fall in client numbers being focused on clients with lower-intensity needs, while the National Audit Office point to demographic factors, such as ageing, increasing the number of clients with high-intensity needs.
In contrast, the cost weighting employed in the output measure will, to an extent, assign a higher cost weight to care for clients with high-intensity needs, and therefore output has not fallen in the same manner as client numbers.
Part of the fall in client numbers may also be due to activity demand management policies – the Local Government Association’s Adult Social Care Efficiency Programme report (PDF, 463.8KB) suggests local authorities have been implementing a number of approaches to diverting lower-need clients away from formal care, such as promoting independence and resilience and offering preventive interventions such as befriending schemes.
On the input side, use of the general GDP deflator results in slightly faster growth overall than experienced by the inputs measure used in productivity, as the specific deflators used in the inputs measure have experienced a greater inflation rate than the general economy over the period.
Client needs
One of the potential drivers of falling productivity is increasing client needs. For instance, higher-need clients in residential care may require more staff time to support and therefore greater input for each week of care provided. To an extent, the public service productivity measure controls for this in residential and nursing care by using separate cost weights for four different client groups in the years until FYE 2014 and six different client groups for the years after FYE 2014. Within the largest element of community care, home care (which is measured using direct activity data until FYE 2014), intensity of need should be partially incorporated into the output measure, as the unit of activity is the number of hours of home care provided and higher-need clients are likely to receive a greater number of hours of home care.
However, within the client groups used in residential and nursing care, and for forms of community care other than home care, there is no further adjustment for additional costs caused by greater client needs.
One source that can be used to analyse changes in client needs is the Adult Social Care Survey (ASCS), which is the data source used for the quality adjustment. More information on the ASCS can be found in Section 8.
The ASCS collects data on the basic activities of daily living (ADLs) clients need support with. Seven categories of ADL support needs are covered, with questions asking whether clients need support to:
move around indoors
get into and out of bed
eat
wash using a bath or shower
get dressed and undressed
use the toilet
wash their face and hands
The ASCS can therefore be used to provide a rough estimate of the intensity of clients’ care needs by examining how many ADLs clients need support with. While some sample weighting has been applied to these figures to account for variations in response by region, caution should be taken when interpreting these figures as clients’ needs may also affect their likelihood of completing the ASCS.
Figures 16 to 19 show how the number of ADLs clients need support with has changed over time, although it should be noted that there is a break in series between FYE 2014 and FYE 2015, due to changes in sample coverage. The changes between these two years means that data up to FYE 2014 are not comparable with data from FYE 2015 onwards.
These figures split the sample by two questionnaires to separate the population completing the main questionnaire and respondents to the “easy-read” questionnaire, which is mainly used by clients with learning disabilities, who typically have fewer ADL support needs.
Figures 16 and 17 suggest there has been little change in the number of ADLs clients in residential and nursing care need support with over the time period. This may suggest that greater intensity of need may not be the main cause of falling productivity in residential and nursing care output, although as previously stated, caution should be taken when drawing firm conclusions from these data.
Figure 16: Number of basic activities of daily living (ADLs) residential and nursing care clients need help with, non-easy read questionnaire
England, financial year ending 2011 to financial year ending 2017
Source: Office for National Statistics
Notes:
There is a break in series between FYE 2014 and FYE 2015.
Percentages may not sum to exactly 100 due to rounding.
Download this chart Figure 16: Number of basic activities of daily living (ADLs) residential and nursing care clients need help with, non-easy read questionnaire
Image .csv .xls
Figure 17: Number of basic activities of daily living (ADLs) residential and nursing care clients need help with, easy-read (learning disability) questionnaire
England, financial year ending 2011 to financial year ending 2017
Source: Office for National Statistics
Notes:
There is a break in series between FYE 2014 and FYE 2015.
Percentages may not sum to exactly 100 due to rounding.
Download this chart Figure 17: Number of basic activities of daily living (ADLs) residential and nursing care clients need help with, easy-read (learning disability) questionnaire
Image .csv .xlsFigures 18 and 19 cover community care. Here a clearer pattern of greater intensity of need over time can be observed, particularly for clients completing the non-easy read questionnaire, where the proportion of clients reporting zero ADL needs decreased, and the proportion of clients reporting seven ADL needs increased, in every year of the period. Comparisons between the period up to FYE 2014 and the period after should again be avoided due to the break in series between these years.
Figure 18: Number of basic activities of daily living (ADLs) community care clients need help with, non-easy read questionnaire
England, financial year ending 2011 to financial year ending 2017
Source: Office for National Statistics
Notes:
There is a break in series between FYE 2014 and FYE 2015.
Percentages may not sum to exactly 100 due to rounding.
Download this chart Figure 18: Number of basic activities of daily living (ADLs) community care clients need help with, non-easy read questionnaire
Image .csv .xls
Figure 19: Number of basic activities of daily living (ADLs) community care clients need help with, easy-read (learning disability) questionnaire
England, financial year ending 2011 to financial year ending 2017
Source: Office for National Statistics
Notes:
There is a break in series between FYE 2014 and FYE 2015.
Percentages may not sum to exactly 100 due to rounding.
Download this chart Figure 19: Number of basic activities of daily living (ADLs) community care clients need help with, easy-read (learning disability) questionnaire
Image .csv .xlsIt should also be noted that the output and productivity of community care is not measured for the years FYE 2015 onwards, as activity data are not available for these years and therefore any change in community care activity or intensity of need will not affect the productivity measures for these later years.
Notes for: Adult social care productivity for England on financial year basis
Activity data for Wales and Northern Ireland are not available and so output for these nations is assumed to grow in line with output for the rest of the UK. Inputs data are also missing for Northern Ireland and so Northern Ireland inputs are assumed to grow in line with inputs for the rest of the UK.
Local authorities pay VAT and NNDR on current expenditure on goods and services, but as HM Revenue and Customs reimburse these payments, the local authorities' own accounts exclude VAT and NNDR. As final consumption is measured at market prices, VAT and NNDR must be added back into local government current expenditure. Current expenditure and reimbursement may not take place in the same year, which would affect the final consumption figures. However, there is no detail available for the period to which VAT and NNDR refunds relate, so the methodology uses VAT and NNDR refunds at time paid. This is therefore a source of differences in year-on-year growth rates between the data used in the UK and data used in the England productivity measures.
11. Additional adult social care productivity measures on an England financial year basis
The change of data source for expenditure in the England financial year productivity measure enables the production of several new productivity measures, including a measure covering only the output for which activity data are available and separate measures by service type and client type.
Productivity for directly measured output
As covered in Section 7, output measured through a cost-weighted activity index is also known as directly-measured output, in contrast with output measured through the “output-equals-inputs” approach, which is known as indirectly-measured output.
While the new adult social care productivity measure provides an improved estimate by aligning the coverage of input and output measures, this is achieved through the incorporation of indirect measures of output through an “output-equals-inputs” element for services where no activity data are available. The implementation of the “output-equals-inputs” element involves an assumption that the productivity change for the element where activity data cannot be measured is zero. Use of this assumption results in the scale of annual changes in productivity being reduced towards zero.
The size of the effect of the “output-equals-inputs” element is proportional to the amount of spending on services covered by the “output-equals-inputs” component.
Figure 20 shows the proportion of output that is produced from directly-measured activity data, with the remainder accounted for by the “output-equals-inputs” component. Figure 20 shows how the “output-equals-inputs” component has grown over time.
Figure 20: Proportion of output directly measured
England, financial year ending 1997 to financial year ending 2017
Source: Office for National Statistics
Notes:
Figures are given as the proportion of output that is directly measured for the purpose of calculating output growth between the stated year and the previous year.
Because output is produced using a Laspeyres index, growth between two years is weighted using data from the first year of each two-year pair. Therefore, as an example, the figure for FYE 2017 refers to the proportion of output that is directly measured for the purpose of calculating output growth between FYE 2016 and FYE 2017, which is calculated from FYE 2016 expenditure data.
Download this chart Figure 20: Proportion of output directly measured
Image .csv .xlsServices covered by the “output-equals-inputs” element from the start of the time series include supported living arrangements and direct payments. The “output-equals-inputs” component grew in financial year ending (FYE) 2004 as a result of the inclusion of a substantial proportion of the Supporting People programme into adult social care (ASC) expenditure. The “output-equals-inputs” component is substantially higher for the years after FYE 2015 due to the reduced coverage of the post-Zero Based Review activity data source.
Productivity growth between FYE 2014 and FYE 2015 was measured entirely on an “output-equals-inputs” basis, in both the main England financial year productivity measure and the direct measures only series, due to the change in activity data source between these years.
Figure 21: Comparison of productivity indices for all services and directly-measured services only, quality adjusted and non-quality adjusted
England, financial year ending 1997 to financial year ending 2017
Source: Office for National Statistics
Download this chart Figure 21: Comparison of productivity indices for all services and directly-measured services only, quality adjusted and non-quality adjusted
Image .csv .xlsFigure 21 shows the two measures diverge more in recent years, because of the increasing size of the “output-equals-inputs” component. The productivity measure for directly-measured services falls more than that of the main England financial year productivity measure, as falls in productivity are not limited by the “output-equals-inputs” component.
Productivity by service type
Use of NHS Digital expenditure data in the input calculations enables new productivity measures to be produced for different service types.
Figures 22, 23 and 24 show inputs, output and productivity for residential and nursing care, community care, and referrals and assessments separately. Due to limitations with the data after the NHS Digital Zero Based Review, the measures for community care, and referrals and assessments end after FYE 2014.
While local authority-provided and independent sector-provided care within each service are deflated separately, separate deflators are not used to calculate inputs for different types of services. Given that different inputs will be required in the provision of different services, the use of the same deflators is an imperfect assumption. However, the analysis of alternative deflators in Section 6 shows only limited differences between alternative deflators for intermediate consumption, suggesting use of more specific deflators for different service types may have a limited effect.
Figure 22 shows the trend in inputs, output and productivity for residential and nursing care. This shows strong growth in both inputs and output between FYE 2002 and FYE 2005, but a decline at an average rate of 1.4% per year for inputs and 2.4% per year for non-quality adjusted output since FYE 2006.
The productivity of residential and nursing care declined between FYE 2004 and FYE 2011 due to the faster rate of fall in output than inputs. Caution should be taken with comparing productivity performance for the period after FYE 2005 to the years before FYE 2005, as payments from the NHS were not included in the measure in the years before FYE 2005.
Figure 22: Public service residential and nursing care; inputs, and quality adjusted and non-quality adjusted output and productivity indices
England, financial year ending 1997 to financial year ending 2017
Source: Office for National Statistics
Download this chart Figure 22: Public service residential and nursing care; inputs, and quality adjusted and non-quality adjusted output and productivity indices
Image .csv .xlsFigure 22 also shows quality adjusted output and productivity. The quality adjustment for residential and nursing care increased by 1.1% in total between FYE 2011 and FYE 2017.
Figure 23 shows inputs, output and productivity for community care. To avoid the community care productivity measure being affected by the large “output-equals-inputs” component of this service, Figure 23 includes directly-measured community care services only, the data on which are available until FYE 2014. Services included in this measure include home care, day care, the provision of equipment and home adaptations, and “meals-on-wheels”.
Removal of the “output-equals-inputs” component does, however, mean that the output and inputs measures used in Figure 23 do not cover all activity in community care.
Figure 23: Public service community care; inputs, and quality adjusted and non-quality adjusted output and productivity indices
England, financial year ending 1997 to financial year ending 2014
Source: Office for National Statistics
Notes:
- The figure covers only services for which activity can be directly measured, and excludes services measured in the overall productivity measures through the “output-equals-inputs” approach.
Download this chart Figure 23: Public service community care; inputs, and quality adjusted and non-quality adjusted output and productivity indices
Image .csv .xlsFigure 23 shows that, in contrast with residential and nursing care, productivity for community services remained relatively stable during the series. One exception is a fall in output and productivity in FYE 2010, which was caused by falling activity across all reported categories of community care. This fall is reflected in changes in activity levels and unit costs in NHS Digital’s publication Personal Social Services Expenditure and Unit Costs – England, 2009-10, particularly for home care and day care.
Figure 24 focuses on the relative changes in productivity of community care, and residential and nursing care following the introduction of the quality adjustment in FYE 2011.
Figure 24: Public service adult social care productivity, quality adjusted and non-quality adjusted, for community care, and residential and nursing care
England, financial year ending 2011 to financial year ending 2017
Source: Office for National Statistics
Notes:
- The figure covers only services for which activity can be directly measured, and excludes services measured in the overall productivity measures through the “output-equals-inputs” approach.
Download this chart Figure 24: Public service adult social care productivity, quality adjusted and non-quality adjusted, for community care, and residential and nursing care
Image .csv .xlsOver the period observed in Figure 24, the quality adjustment for community care experiences greater growth than the adjustment for residential and nursing care. The quality adjustment for community care experienced a total growth of 6.0% between FYE 2011 and FYE 2014, in contrast with a total increase of 0.2% for residential and nursing care between FYE 2011 and FYE 2014, although some caution should be taken in interpreting these differences as the two adjustments are produced using different methods, as outlined in Section 8.
Figure 25 shows the final and smallest element of directly-measured output, referrals to local authority (LA) social care services and assessments to determine what care would be appropriate for clients1. Due to no specific quality adjustment being available for referrals and assessments, only non-quality adjusted productivity is displayed for this measure.
Figure 25: Public service adult social care referrals and assessments; inputs, output and productivity indices
England, financial year ending 1997 to financial year ending 2014
Source: Office for National Statistics
Download this chart Figure 25: Public service adult social care referrals and assessments; inputs, output and productivity indices
Image .csv .xlsFigure 25 shows that the productivity of referrals and assessments declined between FYE 1997 and FYE 2006, as inputs experienced strong growth while output fell slightly before returning to a level similar to FYE 1997 in FYE 2006. This fall in productivity could be due to more extensive activity being carried out in each assessment, although there is limited research available to confirm or disprove this. Between FYE 2006 and FYE 2014, inputs, output and productivity all increased slightly before falling to a level similar to FYE 2006 in FYE 2014.
Productivity of services for older and younger adults
The use of the NHS Digital data also enables the analysis of ASC productivity by client age group. Older adults are defined as those aged 65 and over, while younger adults are aged 18 to 64 years and typically receive social care due to learning disabilities, physical disabilities or mental health needs.
As with the analysis by service type, only input and output relating to services for which activity data are available are included in these productivity measures, meaning they cover residential and nursing care throughout the series and include community care, and referrals and assessments until FYE 2014. This also means that caution should be taken when comparing changes in total input and output volumes for each client group, as these figures exclude services measured on an “output-equals-inputs” basis.
Figure 26 shows the inputs, output and productivity for older adults’ services. This shows that input and output volumes decreased between the mid-2000s and mid-2010s, with output generally falling faster, resulting in falling productivity, although the fall in productivity was slower in the most recent years. In the final year of the series, FYE 2017, this trend experiences a small reversal, with non-quality adjusted output and input volumes growing by 0.3% and 1.6% respectively, and non-quality adjusted productivity falling by 1.3%.
Figure 26: Public service adult social care for older adults: Inputs, and quality adjusted and non-quality adjusted output and productivity indices
England, financial year ending 1997 to financial year ending 2017
Source: Office for National Statistics
Notes:
- The figure covers only services for which activity can be directly measured, and excludes services measured in the overall productivity measures through the “output-equals-inputs” approach.
Download this chart Figure 26: Public service adult social care for older adults: Inputs, and quality adjusted and non-quality adjusted output and productivity indices
Image .csv .xlsFigure 26 also shows quality-adjusted output and productivity for older adults’ services. The quality adjustment increased by 3.7% between FYE 2011 and FYE 2017 and while non-quality adjusted productivity fell by 3.7% between FYE 2011 and FYE 2017, quality adjusted productivity fell by only 0.2%.
Figure 27 shows the inputs, output and productivity for younger adults’ services. Productivity for younger adults’ services fell between FYE 1999 and FYE 2011, firstly as inputs growth exceeded output growth and then as output began to fall as inputs were still increasing.
Following FYE 2011, non-quality adjusted productivity has remained relatively steady, with inputs and non-quality adjusted output falling at similar rates. As with older adults’ services, productivity for younger adults’ services fell in FYE 2017, although in contrast with older adults’ services, the inputs and output of younger adults’ services continued to fall in this year.
Figure 27 also shows the effect of quality adjustment, which increased by 5.9% between FYE 2011 and FYE 2017. Relatively strong quality adjustment growth results in quality-adjusted productivity increasing by 3.3% between FYE 2011 and FYE 2017.
Figure 27: Public service adult social care for younger adults; inputs, and quality adjusted and non-quality adjusted output and productivity indices
England, financial year ending 1997 to financial year ending 2017
Source: Office for National Statistics
Notes:
- The figure covers only services for which activity can be directly measured, and excludes services measured in the overall productivity measures through the “output-equals-inputs” approach.
Download this chart Figure 27: Public service adult social care for younger adults; inputs, and quality adjusted and non-quality adjusted output and productivity indices
Image .csv .xlsFigure 28a compares the productivity performance of older adults’ services with younger adults’ services. This shows a greater fall in productivity for younger adults’ services over the whole series, with most of this fall occurring between the years FYE 2003 to FYE 2011 for both client groups.
Figure 28a: Public service adult social care productivity indices, quality adjusted and non-quality adjusted, for older and younger adults’ services
England, financial year ending 1997 to financial year ending 2017
Source: Office for National Statistics
Notes:
- The figure covers only services for which activity can be directly measured, and excludes services measured in the overall productivity measures through the “output-equals-inputs” approach.
Download this chart Figure 28a: Public service adult social care productivity indices, quality adjusted and non-quality adjusted, for older and younger adults’ services
Image .csv .xlsThis divergent performance may be related to increases in the intensity of care, which could be due to a focus on more intensive care for younger adults or a reduction in service provision for younger adults with lower needs. However, as the Adult Social Care Survey did not exist in the years over which the main divergence in productivity occurred, it is not possible to measure changes in needs or service quality for the different groups.
The proportion of directly-measured activity accounted for by residential and nursing care relative to other services is similar for both age groups over the period to FYE 2014, and so the difference in the proportion of care accounted for by residential and nursing care is unlikely to be responsible for the differing productivity trends for older and younger adults’ services.
Figure 28b: Public service adult social care productivity indices, quality adjusted and non-quality adjusted, for older and younger adults' services
England, financial year ending 2011 to financial year ending 2017
Source: Office for National Statistics
Notes:
- The figure covers only services for which activity can be directly measured, and excludes services measured in the overall productivity measures through the “output-equals-inputs” approach.
Download this chart Figure 28b: Public service adult social care productivity indices, quality adjusted and non-quality adjusted, for older and younger adults' services
Image .csv .xlsFigure 28b focuses on the trends since the introduction of the quality adjustment in FYE 2011. This shows a similar trend in non-quality adjusted productivity between older and younger adults’ services, with non-quality adjusted productivity falling by 3.7% for older adults and falling by 2.4% for younger adults. However, the addition of the quality adjustment results in a greater divergence between the two client groups between FYE 2011 and FYE 2014. Quality-adjusted productivity fell by 0.2% for older adults’ services between FYE 2011 and FYE 2017 and grew by 3.3% for younger adults’ services.
Notes for: Additional adult social care productivity measures on an England financial year basis
- Due to the greater cost and value of care assessments than referrals, assessment activity is given a greater weight in the output.
12. Acknowledgments
The author would like to thank Panos Zerdevas, Jason Snowden and Jacob Maxwell from the Department of Health and Social Care for advice and comments; Julian Forder and Olena Nizalova from the Personal Social Services Research Unit at the University of Kent for advice and quality assurance of the quality adjustment; Anita Charlesworth from the Health Foundation and Garry Young from the National Institute of Economic and Social Research for comments on the publication; the LondonADASS Improvement Programme and Omar Idriss for provision of data on direct payments; and William Laing of LaingBuisson for advice and the provision of data for the deflators.
Nôl i'r tabl cynnwys13. References
Association of Directors of Adult Social Services, ADASS Budget Survey 2017 (PDF, 1.2MB)
Atkinson A (2005), Atkinson Review: Final report – Measurement of Government Output and Productivity for the National Accounts (PDF, 1.1MB)
Care Providers Alliance (2017), Working with care providers to understand costs: A guide for adult social care commissioners (PDF, 640.6KB)
House of Commons Library (2018), Social care: care home market – structure, issues, and cross-subsidisation (England) (PDF, 186KB)
LaingBuisson (2017), Care Cost Benchmarks (eighth edition (PDF, 75KB)
LaingBuisson (2016), Care of Older People (27th edition (PDF, 538.7KB)
Ministry of Housing, Communities and Local Government, Local Authority Revenue Expenditure and Financing
NHS Digital (2017), Adult Social Care Activity and Finance Report, England 2016-17
NHS Digital (2017), Personal Social Services Adult Social Care Survey, England 2016-17
NHS Digital (2017), Measures from the Adult Social Care Outcomes Framework, England – 2016-17
Office for National Statistics (2018), Public service productivity estimates: total public service, UK: 2015
Yang W, Forder J, Nizalova, O (2017), ‘Measuring the productivity of residential long-term care in England: methods for quality adjustment and regional comparison’, Eur J Health Econ, Volume 18, Issue 5, pages 635 to 647
Nôl i'r tabl cynnwys