Cynnwys
- Other pages in this release
- Main points
- Socioeconomic inequalities in avoidable mortality
- Socioeconomic inequalities in avoidable mortality by cause
- The Slope Index of Inequality (SII) in avoidable mortality
- Socioeconomic inequalities in avoidable mortality in Wales data
- Glossary
- Measuring the data
- Strengths and limitations
- Related links
1. Other pages in this release
Socioeconomic inequalities in avoidable mortality in England: 2018
Nôl i'r tabl cynnwys2. Main points
The proportion of total deaths in 2018 that were avoidable in Wales is substantially larger in the most deprived areas compared with the least deprived areas.
Avoidable deaths accounted for two-fifths (40.4%) of all male deaths in the most deprived areas of Wales compared with less than one-fifth (18.1%) in the least deprived areas in 2018; for females it was 26.4% and 10.9% respectively.
While avoidable mortality rates are sizeably lower than they were in 2001 across all levels of area deprivation, since 2013 the speed of improvement has reduced substantially, particularly in the most deprived areas.
Between 2001 and 2018, there was a statistically significant increase in avoidable mortality rates caused by diseases of the respiratory system for males living in the most deprived areas.
The absolute difference in the rate of avoidable death caused by diseases of the circulatory system between the most and least deprived areas of Wales narrowed between 2001 and 2018; the absolute gap widened for diseases of the respiratory system and neoplasms.
The absolute inequality in the rate of avoidable mortality indicated there were 438.5 additional deaths per 100,000 males living in the most deprived areas of Wales compared with the least deprived areas, and 272.9 additional deaths per 100,000 females living in the most deprived areas compared with the least, in 2018.
3. Socioeconomic inequalities in avoidable mortality
Data in this release have been created using the new international avoidable mortality definition (DOC, 421KB). When discussing avoidable deaths, the following terms are used:
preventable mortality - deaths that can be mainly avoided through effective public health and primary prevention interventions
treatable mortality - deaths that can be mainly avoided through timely and effective healthcare interventions, including secondary prevention and treatment
avoidable mortality - deaths defined as either preventable or treatable
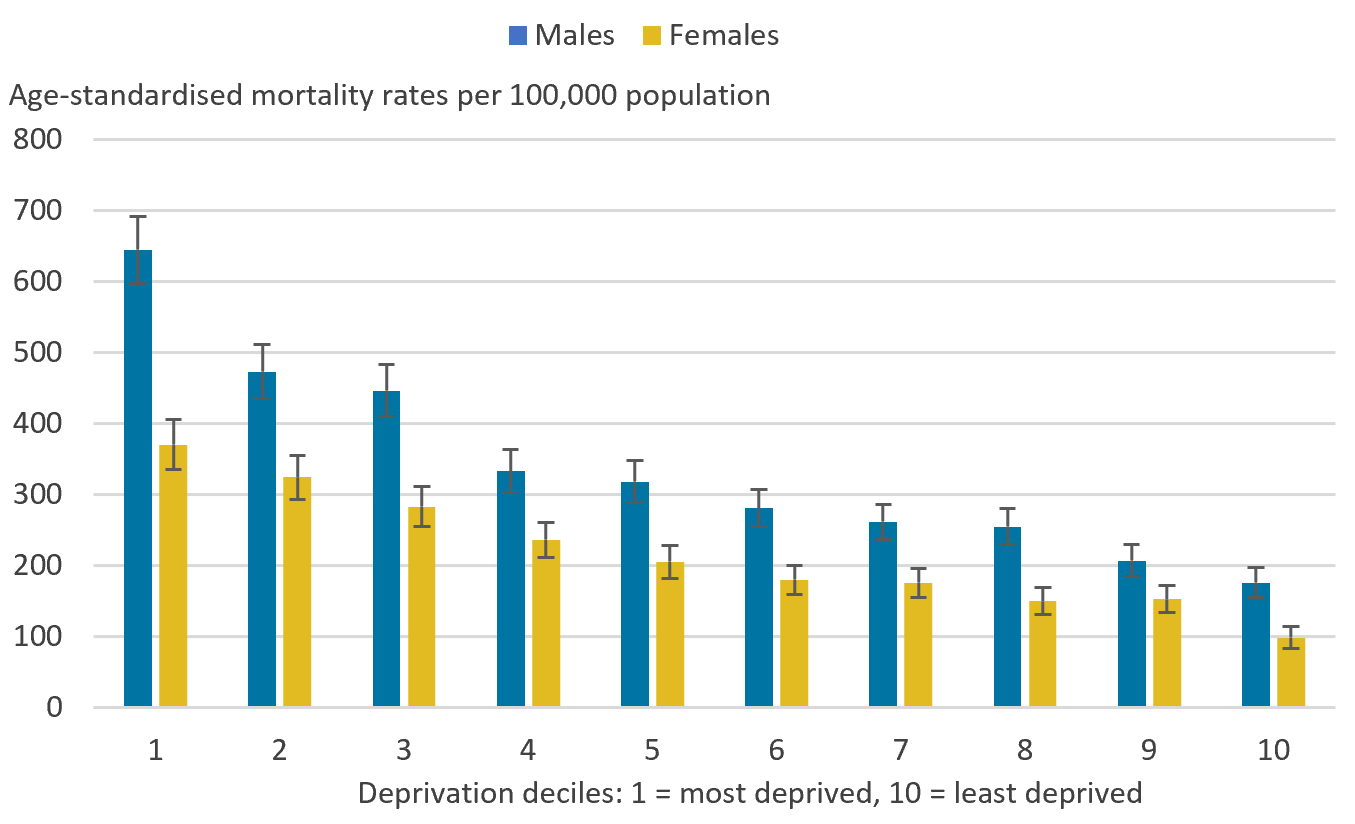
In 2018, the age-standardised avoidable mortality rate for males living in the most deprived areas of Wales (decile 1) was 645.1 deaths per 100,000 males, a statistically significant higher rate than the 176.3 deaths per 100,000 males observed in the least deprived areas (decile 10).
A similar pattern was observed in females, with a statistically significant higher rate for those living in the most deprived areas (370.5 deaths per 100,000 females) compared with the least deprived areas (98.4 deaths per 100,000 females) (Figure 1).
Avoidable mortality rates mostly reduced in a regular pattern as deprivation lessened; for males rates were lower between all subsequent adjacent deciles from decile 1 onwards and for females this was true apart from between deciles 8 and 9. However, these decreases were only statistically significant between deciles 1 and 2 and deciles 3 and 4 for males, and between deciles 9 and 10 for females.
Males living in decile 1 had a statistically significant higher avoidable mortality rate than all other deciles, and those living in decile 10 had a statistically significant lower avoidable mortality rate than eight other deciles. Similarly, for females, those living in decile 1 had a statistically significant higher avoidable mortality rate than eight other deciles, while those living in decile 10 had a statistically significant lower avoidable mortality rate than all other deciles.
The largest absolute gaps were between areas located in decile 1 and 2 for males, and deciles 9 and 10 for females. This demonstrates contrasting avoidable mortality rates even between the most closely aligned populations on the deprivation scale.
When comparing males and females in the same deciles, males had a statistically significant higher avoidable mortality rate than females. However, males exposed to lower levels of deprivation (those living in deciles 6 and higher) had a statistically significant lower rate of avoidable mortality than females living in decile 1.
Figure 1: Males and females living in the most deprived areas had statistically significant higher avoidable mortality rates than those living in the least deprived areas
Age-standardised avoidable mortality rates by sex and decile, Wales, 2018
Source: Office for National Statistics - Deaths registered in Wales
Notes:
- Figures are for deaths registered in 2018.
- Figures for Wales exclude deaths of non-residents.
- Age-standardised mortality rates are expressed per 100,000 population and standardised to the 2013 European Standard Population. Age-standardised mortality rates are used to allow comparison between populations that may contain different proportions of people of different ages.
- Deprivation deciles are based on the Welsh Index of Multiple Deprivation (WIMD), which is the official measure of relative deprivation. 2018 data is based on WIMD 2019.
- Decile 1 represents the most deprived areas and decile 10 represents the least deprived areas.
Download this image Figure 1: Males and females living in the most deprived areas had statistically significant higher avoidable mortality rates than those living in the least deprived areas
.PNG (42.0 kB) .xlsx (18.5 kB)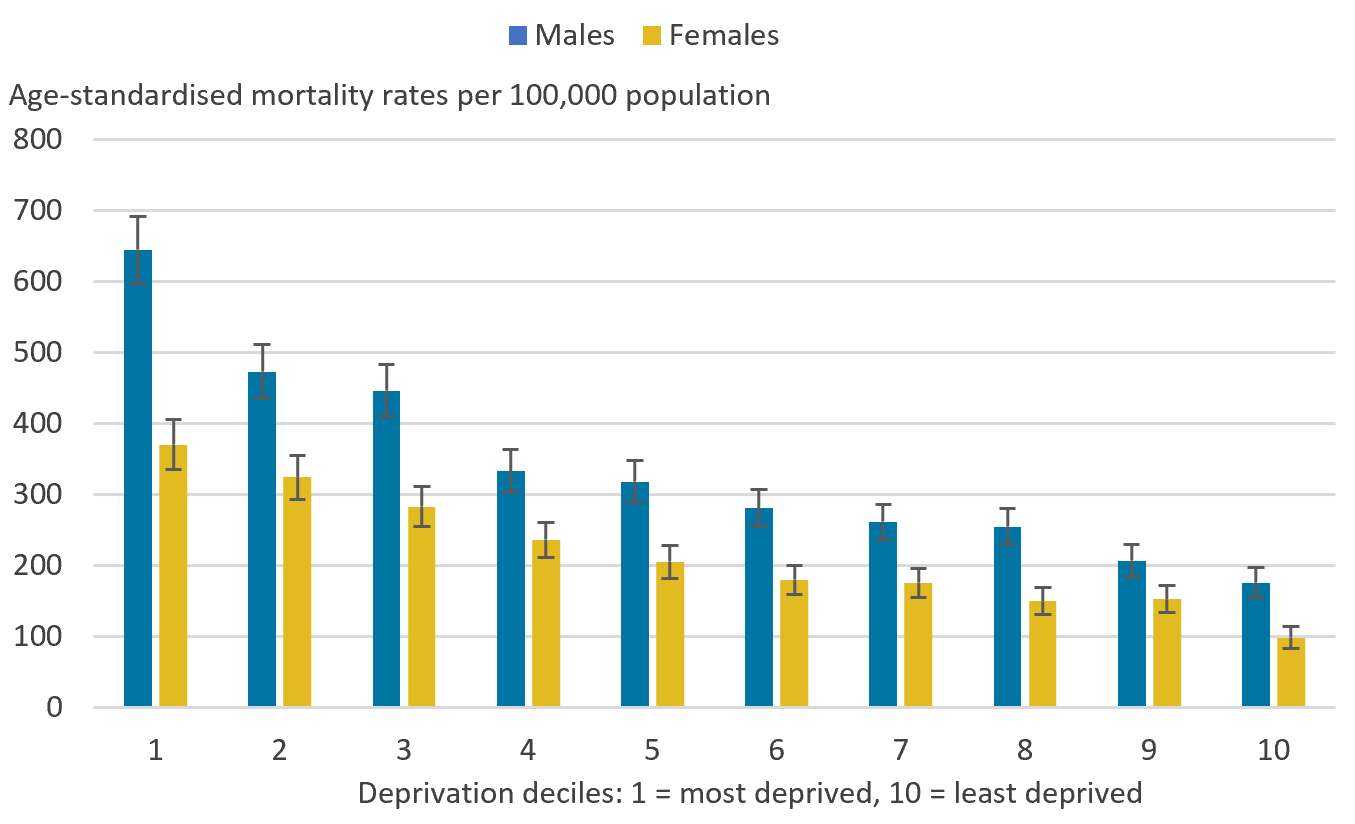{kind=link}
Between 2001 and 2018, avoidable mortality rates statistically significantly decreased for males and females living in the least deprived areas. For those living in the most deprived areas, avoidable mortality rates also decreased between 2001 and 2018, however, these were not statistically significant. In the latest years, increases in avoidable mortality rates were observed particularly for those living in the most deprived areas. This resulted in the absolute gap in avoidable mortality between the most and least deprived areas to be wider in 2018 than in 2001 for both males and females (Figure 2).
Similar to avoidable mortality, treatable mortality rates statistically significantly decreased for males living in the least deprived areas and for females living in both the least and most deprived areas, while statistically significant decreases were only observed in males living in the least deprived areas for preventable mortality. Data for these measures can be found in the accompanying datasets.
Figure 2: Avoidable mortality rates for males and females living in the least deprived areas showed a statistically significant decrease between 2001 and 2018
Age-standardised avoidable mortality rates by sex and selected deciles, Wales, 2001 to 2018
Source: Office for National Statistics - Deaths registered in Wales
Notes:
- Figures are for deaths registered in each calendar year.
- Figures for Wales exclude deaths of non-residents.
- Age-standardised mortality rates are expressed per 100,000 population and standardised to the 2013 European Standard Population. Age-standardised mortality rates are used to allow comparison between populations that may contain different proportions of people of different ages.
- Deprivation deciles are based on the Welsh Index of Multiple Deprivation (WIMD), which is the official measure of relative deprivation. WIMD 2005 was used for data years 2001 to 2004, WIMD 2008 was used for years 2005 to 2007, WIMD 2011 was used for years 2008 to 2010, WIMD 2014 was used for years 2011 to 2014 and WIMD 2019 was used for years 2015 to 2018.
- Decile 1 represents the most deprived areas and decile 10 represents the least deprived areas.
Download this chart Figure 2: Avoidable mortality rates for males and females living in the least deprived areas showed a statistically significant decrease between 2001 and 2018
Image .csv .xlsFigure 3 illustrates the improvements in avoidable mortality rates across three discrete time periods spanning six years: 2001 and 2006, 2007 and 2012 and 2013 and 2018. For males and females living in the most and least deprived areas, the greatest improvements in avoidable mortality rates were observed between 2007 and 2012, the largest of which was observed in those living in the least deprived areas.
In contrast, the percentage change between 2013 and 2018 for those living in the most deprived areas worsened with a 10.6% increase in male avoidable deaths and an 18.6% increase for females. These increases contributed to the widening of the absolute gap between those living in the most and least deprived areas of Wales.
These findings support and are consistent with the marked slowdown of improvement in mortality rates in the latest period, previously reported in the recent changing trends in mortality analysis and health state life expectancy by national deprivation deciles releases. These findings also show that even in periods where avoidable mortality was reducing quickly, rates reduced more quickly in the least deprived areas compared with the most.
Figure 3: Improvements in avoidable mortality rates were greatest between 2007 and 2012 for males and females living in the most and least deprived areas
Percentage change in age-standardised avoidable mortality rates by sex and selected deciles, Wales, between 2001 and 2006, 2007 and 2012, and 2013 and 2018
Source: Office for National Statistics - Deaths registered in Wales
Notes:
- Percentage change in avoidable mortality is calculated by subtracting the earlier mortality rate from the later mortality rate for each time period, before dividing by the earlier mortality rate. This is expressed as a percentage.
- Figures are for deaths registered in each calendar year.
- Figures for Wales exclude deaths of non-residents.
- Deprivation deciles are based on the Welsh Index of Multiple Deprivation (WIMD), which is the official measure of relative deprivation. WIMD 2005 was used for data years 2001 to 2004, WIMD 2008 was used for years 2005 to 2007, WIMD 2011 was used for years 2008 to 2010, WIMD 2014 was used for years 2011 to 2014 and WIMD 2019 was used for years 2015 to 2018.
- Decile 1 represents the most deprived areas and decile 10 represents the least deprived areas.
Download this chart Figure 3: Improvements in avoidable mortality rates were greatest between 2007 and 2012 for males and females living in the most and least deprived areas
Image .csv .xls4. Socioeconomic inequalities in avoidable mortality by cause
Causes of avoidable mortality can be categorised into seven broad cause groups. This section has focused on three of these broad causes:
diseases of the circulatory system
diseases of the respiratory system
neoplasms
These causes differ to those covered in the England-specific bulletin because death counts are smaller in Wales, which means complete time series were not available for all broad causes. Data for broad cause groups are available in the accompanying datasets.
Diseases of the circulatory system
Between 2001 and 2018, avoidable mortality rates for diseases of the circulatory system statistically significantly declined for males and females living in the most and least deprived areas of Wales (Figure 4). The largest absolute decreases were observed in those living in the most deprived areas, with decreases of 115.7 deaths per 100,000 males and 89.2 deaths per 100,000 females.
In comparison, the absolute decreases for those living in the least deprived areas were 97.0 deaths per 100,000 males and 39.1 deaths per 100,000 females. These overall decreases led to the absolute gap between the most and least deprived areas narrowing between 2001 and 2018.
Despite avoidable mortality rates for diseases of the circulatory system showing a marked statistically significant decrease between 2001 and 2018 for both the most and least deprived areas, in 2018 they remained statistically significantly higher for those living in the most deprived areas compared with the least deprived areas (4.1 times higher for males and 4.9 times higher for females). Additionally, avoidable mortality rates for males remain statistically significantly higher than females living in the same decile.
Between 2001 and 2011, avoidable mortality rates for males and females living in the most and least deprived areas generally declined year-on-year with overall statistically significant decreases. However, between 2011 and 2018 a notable slowdown in improvement was observed with overall non-significant changes.
Figure 4: Avoidable mortality rates decreased for diseases of the circulatory system between 2001 and 2018 in the most and least deprived areas
Age-standardised avoidable mortality rates for diseases of the circulatory system by sex and selected deciles, Wales, 2001 to 2018
Source: Office for National Statistics - Deaths registered in Wales
Notes:
- Figures are for deaths registered in each calendar year.
- Figures for Wales exclude deaths of non-residents.
- Age-standardised mortality rates are expressed per 100,000 population and standardised to the 2013 European Standard Population. Age-standardised mortality rates are used to allow comparison between populations that may contain different proportions of people of different ages.
- Deprivation deciles are based on the Welsh Index of Multiple Deprivation (WIMD), which is the official measure of relative deprivation. WIMD 2005 was used for data years 2001 to 2004, WIMD 2008 was used for years 2005 to 2007, WIMD 2011 was used for years 2008 to 2010, WIMD 2014 was used for years 2011 to 2014 and WIMD 2019 was used for years 2015 to 2018.
- Decile 1 represents the most deprived areas and decile 10 represents the least deprived areas.
Download this chart Figure 4: Avoidable mortality rates decreased for diseases of the circulatory system between 2001 and 2018 in the most and least deprived areas
Image .csv .xlsDiseases of the respiratory system
Avoidable mortality rates for diseases of the respiratory system were sharply contrasting between those living in the most and least deprived areas of Wales with rates 4.4 times higher for males and 7.0 times higher for females in 2018 (Figure 5).
Between 2001 and 2018, avoidable mortality rates for males living in the most deprived areas have fluctuated with an overall statistically significant increase from 67.9 deaths per 100,000 males to 106.0 deaths per 100,000 males.
Avoidable mortality rate increases were also observed for males living in the least deprived areas and females living in the most deprived areas, however these were not statistically significant. Avoidable mortality rates for females living in the least deprived areas non-significantly decreased. These increases resulted in the absolute gap between those living in the most and least deprived areas to be wider in 2018 than 2001.
The widening of the absolute gap indicates a lack of health improvement in these diseases causing the inequality to grow. The substantially higher rates observed in the most deprived areas compared with the least deprived areas can be linked to differential smoking prevalence and exposure to air pollution, both of which are higher in more deprived areas, and these two factors combined have a role in increasing risk of respiratory-related mortality.
Figure 5: The gap between avoidable mortality rates for diseases of the respiratory system between the most and least deprived areas was wider in 2018 than 2001
Age-standardised avoidable mortality rates for diseases of the respiratory system by sex and selected deciles, Wales, 2001 to 2018
Source: Office for National Statistics - Deaths registered in Wales
Notes:
- Figures are for deaths registered in each calendar year.
- Figures for Wales exclude deaths of non-residents.
- Age-standardised mortality rates are expressed per 100,000 population and standardised to the 2013 European Standard Population. Age-standardised mortality rates are used to allow comparison between populations that may contain different proportions of people of different ages.
- Deprivation deciles are based on the Welsh Index of Multiple Deprivation (WIMD), which is the official measure of relative deprivation. WIMD 2005 was used for data years 2001 to 2004, WIMD 2008 was used for years 2005 to 2007, WIMD 2011 was used for years 2008 to 2010, WIMD 2014 was used for years 2011 to 2014 and WIMD 2019 was used for years 2015 to 2018.
- Decile 1 represents the most deprived areas and decile 10 represents the least deprived areas.
Download this chart Figure 5: The gap between avoidable mortality rates for diseases of the respiratory system between the most and least deprived areas was wider in 2018 than 2001
Image .csv .xlsNeoplasms
Between 2001 and 2018, avoidable mortality rates for deaths caused by neoplasms have remained statistically significantly higher for those living in the most deprived areas compared with the least deprived areas (Figure 6).
Avoidable mortality rates for neoplasms have fluctuated throughout the time series with overall decreases for those living in the most and least deprived areas of Wales; however, only the decrease observed for females living in the least deprived areas was statistically significant. These mostly non-significant decreases and fluctuations across the time series produced an increase in the absolute gap between those living in the most and least deprived areas of Wales by 2018.
Figure 6: The gap between avoidable mortality rates for neoplasms between the most and least deprived areas was wider in 2018 than 2001
Age-standardised avoidable mortality rates for neoplasms by sex and selected deciles, Wales, 2001 to 2018
Source: Office for National Statistics - Deaths registered in Wales
Notes:
- Figures are for deaths registered in each calendar year.
- Figures for Wales exclude deaths of non-residents.
- Age-standardised mortality rates are expressed per 100,000 population and standardised to the 2013 European Standard Population. Age-standardised mortality rates are used to allow comparison between populations that may contain different proportions of people of different ages.
- Deprivation deciles are based on the Welsh Index of Multiple Deprivation (WIMD), which is the official measure of relative deprivation. WIMD 2005 was used for data years 2001 to 2004, WIMD 2008 was used for years 2005 to 2007, WIMD 2011 was used for years 2008 to 2010, WIMD 2014 was used for years 2011 to 2014 and WIMD 2019 was used for years 2015 to 2018.
- Decile 1 represents the most deprived areas and decile 10 represents the least deprived areas.
Download this chart Figure 6: The gap between avoidable mortality rates for neoplasms between the most and least deprived areas was wider in 2018 than 2001
Image .csv .xls5. The Slope Index of Inequality (SII) in avoidable mortality
The Slope Index of Inequality (SII) is used to assess the absolute inequality in avoidable mortality and represents the difference between the hypothetical "most" and "least" deprived areas on the deprivation scale taking into account inequality across all adjacent deciles.
Between 2001 and 2018, the inequality in the male avoidable mortality rate showed a non-significant increase from 418.5 deaths per 100,000 males to 438.5 deaths per 100,000 males (Figure 7). Specifically, this indicates that in 2018 there were 438.5 additional deaths per 100,000 males living in the most deprived areas of Wales compared with the least deprived areas.
Like males, the inequality in the female avoidable mortality rate showed a non-significant increase from 267.3 deaths per 100,000 females in 2001 to 272.9 deaths per 100,000 females in 2018, which indicates a total of 272.9 additional deaths per 100,000 females living in the most deprived areas of Wales compared with the least deprived areas.
Overall, while there has been health improvement in avoidable mortality across all levels of deprivation since 2001, these findings highlight the scale of absolute gaps between the most and least deprived areas of Wales have remained entrenched. In fact, since 2013, there has been a consistent pattern of avoidable mortality inequality rising in Wales for both males and females.
Figure 7: The Slope Index of Inequality (SII) for males and females increased between 2001 and 2018 for avoidable mortality
Trend in the Slope Index of Inequality (SII) for avoidable mortality by sex, Wales, 2001 to 2018
Source: Office for National Statistics - Deaths registered in Wales
Notes:
- Figures are for deaths registered in each calendar year.
- Figures for Wales exclude deaths of non-residents.
- The Slope Index of Inequality (SII) is reported as a positive value to demonstrate increasing mortality rates with increasing deprivation. However, because the relative rank ranges from 0 (most deprived) to 100 (least deprived) the actual SII is negative.
Download this chart Figure 7: The Slope Index of Inequality (SII) for males and females increased between 2001 and 2018 for avoidable mortality
Image .csv .xls6. Socioeconomic inequalities in avoidable mortality in Wales data
Socioeconomic inequalities in avoidable mortality: Wales analysis
Dataset | Released 10 July 2020
Annual age-standardised mortality rates by deprivation decile, sex and cause as well as absolute (Slope Index of Inequality) measures of inequality in Wales.
7. Glossary
Preventable mortality
Preventable mortality refers to causes of death that can be mainly avoided through effective public health and primary prevention interventions (that is, before the onset of diseases or injuries, to reduce incidence).
Treatable mortality
Treatable mortality refers to causes of death that can be mainly avoided through timely and effective healthcare interventions, including secondary prevention and treatment (that is, after the onset of disease, to reduce case-fatality).
Avoidable mortality
Avoidable mortality refers to deaths that are preventable or treatable.
Statistical significance
The term "significant" refers to statistically significant changes or differences. Significance is determined by the 95% confidence intervals, where non-overlapping confidence intervals between figures demonstrate that the difference is unlikely to be because of random fluctuation.
Age-standardised mortality rates
Age-standardised mortality rates are used to allow comparisons between populations, which may contain different proportions of people of different ages.
Slope Index of Inequality (SII)
The SII models the absolute inequality (the difference between the hypothetical most and least deprived populations) in avoidable mortality using weighted linear regression, which takes account of the inequality across all adjacent deciles of relative deprivation, rather than focusing only on the differencing of the two extremes.
Nôl i'r tabl cynnwys8. Measuring the data
This article looks at the socioeconomic inequalities in avoidable mortality in Wales from 2001 to 2018. The analyses use age-standardised mortality rates by deprivation decile, sex and cause as well as absolute (Slope Index of Inequality) measures of inequality. Figures are calculated using death registration data for Wales held by the Office for National Statistics (ONS).
Defining avoidable mortality
With advances in medical technology and wider public health interventions, deaths from conditions previously not avoidable may have since become avoidable. This means the avoidable mortality definition requires review and, if appropriate, revisions.
In 2017, an Organisation for Economic Co-operation and Development (OECD) working group was set up to review the definitions of avoidable mortality used internationally with a remit to create a harmonised definition. The group proposed a new definition of avoidable mortality (PDF, 688KB) and in 2019, the ONS ran a public consultation (DOC, 730KB) to review this definition. As a result of the consultation, it was agreed the ONS would implement the new international avoidable mortality definition (DOC, 421KB) to ensure our statistics are comparable. The new definition has been implemented from data year 2001 onwards. Please note that under the new avoidable mortality definition, there is an upper age limit of 74 years for all causes of death.
Our definition of avoidable mortality is different to the measure of avoidable deaths in hospital, which NHS Trusts in England are required to publish figures on. We use a defined set of underlying causes of death that have been approved through consultation with users and expert guidance. It includes conditions where it is reasonable to expect deaths to be avoided through good quality healthcare, even after the condition has developed (treatable mortality), as well as those where it is possible to prevent the condition from occurring in the first place (incidence reduction) through wider public health interventions, such as those targeted at reducing the incidence of smoking (preventable mortality).
The avoidable deaths in hospital measure is based on a record review of a sample of deaths deemed to be the result of problems in care. Avoidable deaths in hospital data are not intended to be comparable and are not currently collated centrally.
Socioeconomic deprivation
Socioeconomic deprivation is measured using the Welsh Index of Multiple Deprivation (WIMD), which provides an overall relative measure of deprivation for each Lower layer Super Output Area (LSOA). An LSOA is a small area with an average population of 1,500 people. The overall deprivation scores are ranked for all LSOAs within a country and can be divided into 10 groups (deciles) where decile 1 represents the most deprived LSOAs and decile 10 represents the least deprived LSOAs. The IMD is a score based on the area as a whole and not everyone within a LSOA necessarily experiences the same level or type of deprivation.
Different versions of the WIMD were used for this time series:
WIMD 2005 was used for data years 2001 to 2004
WIMD 2008 was used for data years 2005 to 2007
WIMD 2011 was used for data years 2008 to 2010
WIMD 2014 was used for data years 2011 to 2014
WIMD 2019 was used for data years 2015 to 2018
Early access for quality assurance purposes
We provide early access for quality assurance to a small number of people working in other government bodies. This is for general comment on the plausibility of our findings. However, the ONS itself independently produces these statistics, including determining the focus, content, commentary, illustration and interpretation of the measures presented in this article.
More quality and methodology information on strengths, limitations, appropriate uses, and how the data were created is available in the Socioeconomic inequalities in avoidable mortality QMI.
Nôl i'r tabl cynnwys9. Strengths and limitations
The strengths of the socioeconomic inequalities in avoidable mortality bulletin include:
data are compiled using information supplied when a death is registered, which gives complete population coverage and ensures the estimates are of high precision and representative of the underlying population at risk
coding for cause of death is carried out according to the World Health Organization (WHO) International Classification of Diseases ICD-10 and internationally agreed rules
the implementation of the new international avoidable mortality definition (PDF, 421KB) means our statistics are internationally comparable
The limitations of the socioeconomic inequalities in avoidable mortality bulletin include:
in a very small number of cause of death breakdowns, the number of deaths is either too small to report an age-standardised rate or too small to report a rate with reliability; it is our practice not to calculate rates based on fewer than 10 deaths and rates based on 10 to 19 deaths are marked with a "u" to warn users that their reliability is low
provisional data was not used for this article therefore the time series is not fully up to date