1. Introduction
For the first time, this article reports Experimental Statistics on deaths in prison custody based on National Statistics definitions of deaths caused by suicide and drug-related poisoning. Experimental Statistics are those that are in the testing phase and not yet fully developed.
In England and Wales, “deaths in prison custody” means any death of a person arising from an incident occurring during (or, on rare occasions, immediately prior to) prison custody, and also includes deaths of those while released on temporary licence (ROTL) on medical grounds. Prison custody (PDF, 245KB) includes all public and contracted prison establishments and escort contractors.
The Ministry of Justice (MoJ) reports official estimates of deaths, in their Safety in custody statistics, with reference to broad, and often provisional, cause of death groups. The groups include “self-inflicted deaths”, defined as any death of a person who has taken their own life irrespective of intent – which includes suicides and also accidental deaths as a result of the person’s own actions.
What’s included in this analysis?
This article aims to provide further detail on self-inflicted deaths in prison custody, with a particular focus on suicide and drug-related deaths, using data held by the Office for National Statistics (ONS) according to National Statistics definitions.
Due to the growing concern about the level of drug use in prison, for the first time, this analysis aims to provide evidence of drug-related deaths in prisons as this is not included in MoJ’s publication. It is important to note that due to the overlap in our definitions, drug-related deaths are also counted within our definition of suicide where they are classified as self-poisoning (either intentional or undetermined intent). Please see Section 7 of this article, Sources of data used in this analysis for further information on our definitions.
The article aims to improve coherence across government statistics on self-inflicted deaths in prison custody. The analysis covers:
the risk of suicide in the prison population and how this compares with the general population; for these deaths we also describe high-level findings on suicide method
the risk of drug-related death in the prison population and how this compares with the general population; for these deaths we also describe the substances that contributed to the death
how the cause of death assigned by the MoJ compares with that assigned by the ONS
registration delays; the time between the date of death and its eventual registration after inquest
Males make up the large majority of the prison population and therefore the vast majority of deaths in prison custody are among males. Unless stated otherwise, our analyses are presented for men only as reliable results cannot be produced for females due to small numbers.
How did we approach the analysis?
The ONS holds data for all deaths registered in England and Wales. We only have the information that an individual died in prison custody if the death was recorded as taking place in a prison or if this information was provided by the coroner in their inquest report.
For greater robustness, we identified those who had died in prison custody by linking records in our death registrations database with records held by the MoJ in Her Majesty’s Prison and Probation Service (HMPPS) Deaths in custody database.
Nôl i'r tabl cynnwys2. Main points
We identified 1,830 deaths in prison custody from 2008 to 2016 in our death registrations database after linking with the HM Prison and Probation Service (HMPPS) Deaths in custody database; equivalent to around 200 deaths a year, with the majority of deaths being among males (97%).
462 of the identified deaths in males and females were caused by suicide and 88 were drug-related deaths as defined using our National Statistics definitions.
Male prisoners were at an increased risk of dying by suicide compared with the general male population; the risk of male prisoners dying by suicide was 3.7 times higher than the general male population during the nine-year period.
The large majority (93%) of all suicide deaths in prison custody between 2008 and 2016 were caused by hanging, strangulation and suffocation.
The risk of male prisoners dying from drug-related causes was similar to the general male population; opiates were the most common drug type mentioned on death certificates (62 mentions), with methadone, and heroin and morphine being the most common forms.
3. Information guidance
Information for the media
If you are a journalist covering a suicide-related issue, please consider following the Samaritans’ media guidelines on the reporting of suicide, due to the potentially damaging consequences of irresponsible reporting. In particular, the guidelines advise on terminology and include links to sources of support for anyone affected by the themes in the article, such as Samaritans.
Where to go for help
If you are struggling to cope, please call Samaritans free on 116 123 (UK and Ireland), email jo@samaritans.org, or visit the Samaritans website to find details of the nearest branch. Samaritans is available round the clock, every single day of the year, providing a safe place for anyone struggling to cope, whoever they are, however they feel, whatever life has done to them.
Nôl i'r tabl cynnwys4. Things you need to know about this release
This article describes data on deaths caused by suicide or drug-related causes that took place in England and Wales between 2008 and 2016 while an individual was in prison custody.
The analysis is based on death registrations data held by the Office for National Statistics (ONS) linked with data on deaths in prisons provided by the Ministry of Justice (MoJ). Although the MoJ publishes more timely data as part of their Safety in custody statistics, the figures presented here are limited to 2016 due to the delays in some of these deaths being registered. The ONS only receives information on deaths in prison custody following the conclusion of the coroner’s inquest.
Unlike other ONS mortality publications that are based on the date of death registration, the findings in this article are based on the date of death, referred to as occurrence, to improve comparability with Safety in custody statistics.
Data used in the analysis
The ONS holds data on all deaths registered in England and Wales. To identify those who died in prison custody, we linked records held by the MoJ in the HM Prison and Probation Service (HMPPS) Deaths in custody database with records from our death registrations database. Our analyses are for those aged 15 years and above and include those we successfully identified in our death registrations data following data linkage.
More detailed information on each data source and the linkage can be found in Section 8 of this article, Data linkage.
Data analysis
In this article, most of our findings are presented as standardised mortality ratios (SMRs). This commonly used measure of mortality, for the purpose of this analysis, establishes whether the rate of suicides or drug-related poisonings in the male prison population was high or low relative to patterns of risk, for these two causes, in the equivalent general population of England and Wales (that is, all men in England and Wales aged 15 years and above) by taking into account the differences in the age and sex structure between the prison and general populations.
An SMR higher than 100 indicates a greater risk among the male prison population for a given cause of death; values lower than 100 suggest lower than expected risk (for example, an SMR of 150 means a 50% increase in the risk among the prison population, compared with people of the same age and sex group in the population). The SMR should not be used to understand how the level of risk changes over time; for this purpose, we have also included age-standardised rates.
In the analysis, the population at risk was defined using available prison custody population data (XLS, 621KB), and due to the small number of deaths we report our findings using three-year rolling periods. Using three-year rolling periods helps to smooth out fluctuations over time, however, the mortality rate in any given time period will be influenced by those in the preceding years.
More detailed information on the analytical approach including the SMR can be found in Section 9 of this article, Data analysis.
Nôl i'r tabl cynnwys5. Limitations of the analyses
The figures in this article have been produced as Experimental Statistics, which are in the testing phase and not yet fully developed. Official estimates of self-inflicted deaths in prisons should be taken from Safety in custody statistics.
The analysis is based only on deaths that occurred during the period between 2008 and 2016, which we were able to link (1,830 out of the 2,040 records provided by the Ministry of Justice (MoJ) during the period or 90%). Furthermore, it is likely that our findings underestimate the level of risk due to registration delays, as the analysis is based on the date of death. This is particularly the case for the most recent period (2014 to 2016), which we flag in this article as being preliminary.
Data reported in this article are less timely than those reported in Safety in custody statistics. Due to registration delays, we are unable at the time of analysis to provide estimates after 2016 due to not yet having sufficiently complete registration of such deaths occurring more recently. Please see Section 7 of this article, Sources of data used in this analysis for further information.
Nôl i'r tabl cynnwys6. Results
We identified a total of 1,830 deaths in prison custody from 2008 to 2016 in our death registrations database after linking with HM Prison and Probation Service (HMPPS) Deaths in custody database. With males comprising around 95% of the prison population (XLS, 621KB), the majority of these were male deaths, which accounted for 97% of all deaths (1,768) compared with 62 female deaths (3%) over this nine-year period.
Of these deaths, 462 (males and females) were caused by suicide and 88 were drug-related deaths, as defined using our National Statistics definitions. Due to the overlap in our definitions, 12 of the 88 drug-related deaths are also counted within our definition of suicide as they were classified as self-poisoning (either intentional or undetermined intent). Most other deaths fell into the categories of diseases of the circulatory system (International Classification of Diseases ICD-10 codes I00 to I99; 428 deaths) and neoplasms (ICD-10 codes C00 to D48; 398 deaths). A full breakdown of cause of death by ICD chapter can be found in the accompanying reference tables.
The findings presented in this section focus on deaths from suicide and drug-related causes in the male prison population. We were unable to provide analysis for the female prison population due to small numbers of deaths. The risk of males dying by suicide and drug-related deaths in prison custody is compared with the general male population using the standardised mortality ratio (SMR) whilst age-standardised rates are presented to allow comparisons over time.
Suicide deaths in prison custody
During the period 2008 to 2016, there were 462 suicide deaths in prison custody in England and Wales. The large majority were male deaths, which accounted for 97% of all suicides (450 deaths) compared with 12 female deaths over this nine-year period.
This equates to approximately 51 deaths caused by suicide each year.
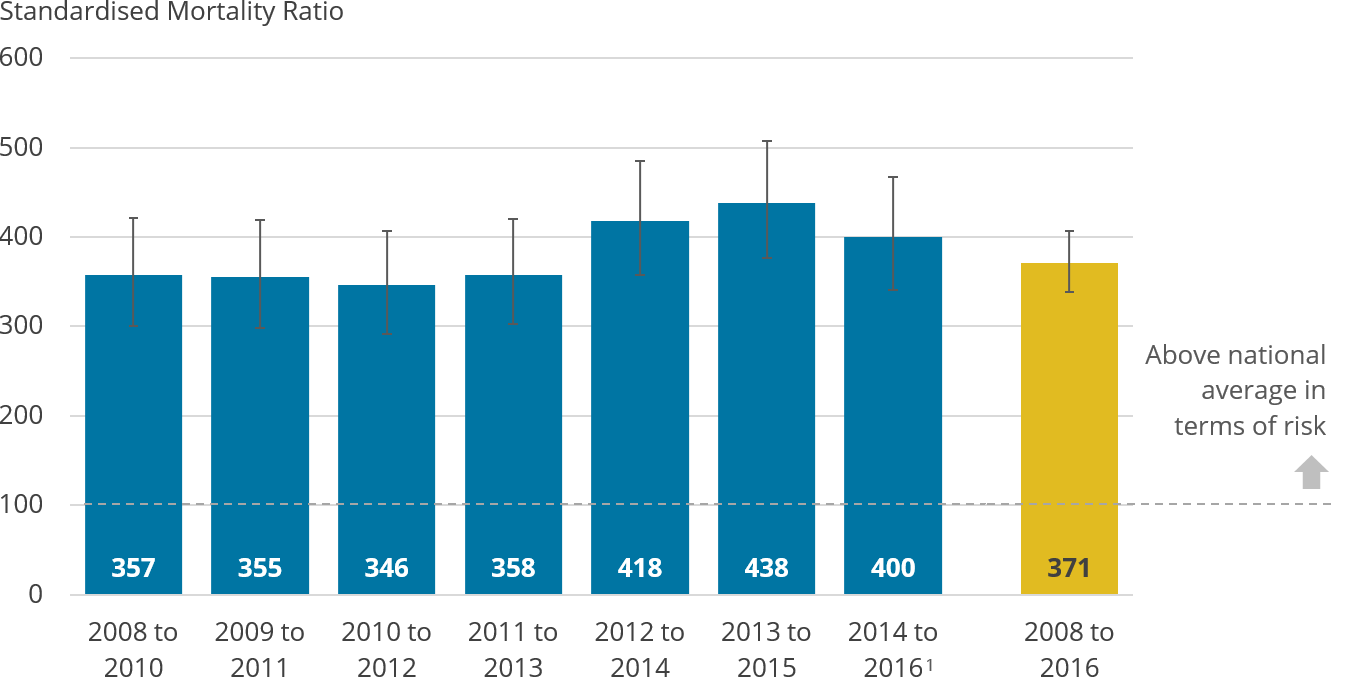
There was a significantly higher risk of suicide in the male prison population compared with the general male population, with the risk of suicide in the male prison population being 3.7 times higher during the entire period (see Figure 1).
It is important to note that while our analyses account for some risk factors that are overrepresented in the prison population (PDF, 228KB) (age and sex), it does not reflect others (for example, a history of mental health problems or substance misuse). As a result, the comparison should not be seen as indicating that there is an increased risk of suicide associated specifically with prison custody.
These findings are similar to those published by the Ministry of Justice (MoJ) that found elevated levels of risk among the prison population for self-inflicted deaths (PDF, 293KB). It is likely that the dip in the most recent estimate for 2014 to 2016 is due to not all of the deaths in this period being registered at the time of analysis.
Figure 1: Male prisoners are at a higher risk of dying by suicide compared with the general population
Suicide death occurrences in prison custody in 2008 to 2016, standardised mortality ratios, males, England and Wales
Source: Office for National Statistics
Notes:
- Estimates for 2014 to 2016 are expected to be an underestimate and should be interpreted with caution.
- Figures are based on the National Statistics definition of suicide for the year the death occurred. Figures are for males aged 15 years and over.
- The standard mortality ratio (SMR) is a common measure of mortality. The dashed line represents the level of suicide among the general male population in England and Wales (SMR equals 100). When the value of the SMR per period is above 100, the risk of suicide is higher in the male prison population compared with peers of the same age group and sex in the population.
- Error bars show the upper and lower confidence limits, which is a margin of error around the SMR estimates. When the range of the upper and lower confidence intervals exclude 100, the risk of suicide for a given period is statistically different to that observed in the general male population of England and Wales.
Download this image Figure 1: Male prisoners are at a higher risk of dying by suicide compared with the general population
.png (37.3 kB) .xls (45.6 kB)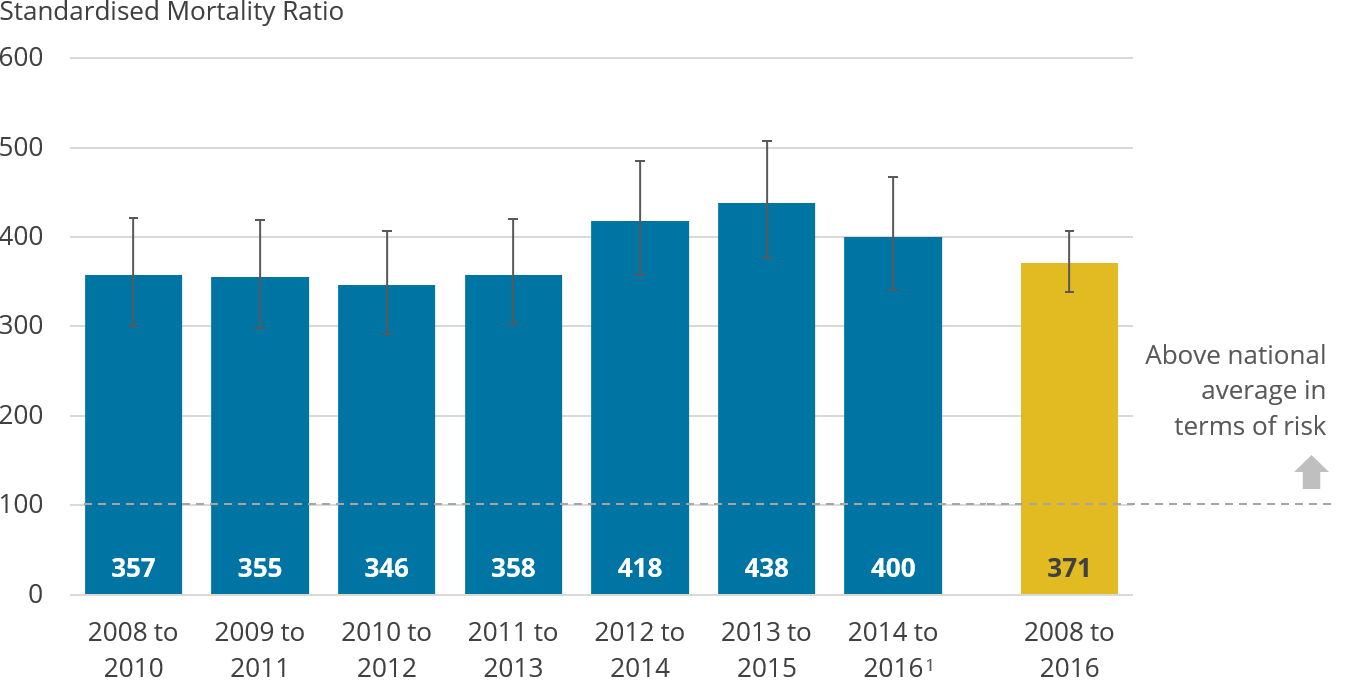{kind=link}
Across the time series, the rate of suicide has remained significantly higher in the male prison population compared with males in the general population (see Figure 2).
Whilst Figure 2 shows apparent changes in the rate of suicide in the male prison population over time, no statistically significant changes can be identified. This is due to the relatively small number of deaths creating a greater degree of statistical uncertainty as reflected in the wide confidence intervals reported in the accompanying dataset.
Figure 2: The rate of suicide in the male prison population remains consistently higher than the general male population over time
Age-standardised male suicide rates, England and Wales, 2008 to 2016
Source: Office for National Statistics
Notes:
- Estimates for 2014 to 2016 are expected to be an underestimate and should be interpreted with caution.
- Figures are based on the National Statistics definition of suicide for the year the death occurred. Figures are for males aged 15 years and over.
- Age-standardised suicide rates per 100,000 population, standardised to the 2013 European Standard Population (ESP). Age-standardised rates are used to allow comparison between populations that may contain different proportions of males of different ages.
Download this chart Figure 2: The rate of suicide in the male prison population remains consistently higher than the general male population over time
Image .csv .xlsSuicide method
The most common method of suicide among the prison population, including both males and females, was by hanging, strangulation and suffocation, which accounted for 93% (430 deaths) of all suicide deaths in prison custody during 2008 to 2016.
Deaths caused by poisoning accounted for 3% (12 deaths) of all suicide deaths in the prison population, whilst a further 4% were categorised as “other”, which largely consisted of suicides caused by intentional self-harm by a sharp object.
In the general population, the proportion of suicides caused by hanging, strangulation and suffocation, during the same period, was 54%, and for poisonings 22%.
Drug-related deaths in prison custody
During the period 2008 to 2016, there were 88 drug-related deaths in prison custody. The large majority were male deaths, which accounted for 93% of all drug-related deaths (82 deaths) compared with six female deaths over this nine-year period.
This equates to almost 10 drug-related deaths in prison custody each year.
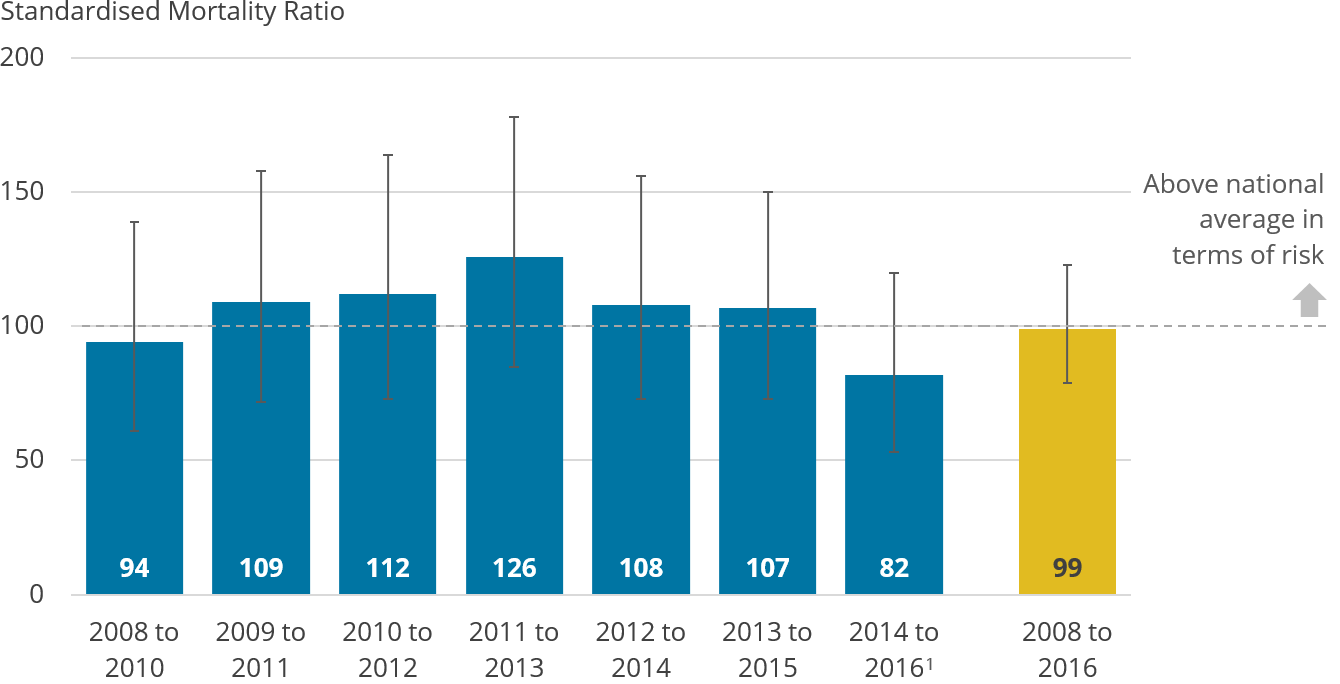
The risk of dying by drug poisoning in the male prison population was not significantly higher or lower than the general male population in England and Wales, as shown in Figure 3.
It is important to note that while our analyses account for some risk factors that are overrepresented in the prison population (age and sex), it does not reflect others (for example, a history of mental health problems or substance misuse).
Figure 3: The risk of drug-related deaths in the male prison population is comparable with the male general population
Drug-related death occurrences in prison custody in 2008 to 2016, standardised mortality ratios, males, England and Wales
Source: Office for National Statistics
Notes:
- Estimates for 2014 to 2016 are expected to be an underestimate and should be interpreted with caution.
- Figures are based on the National Statistics definition of drug-related deaths for the year the death occurred. Figures are for males aged 15 years and over.
- The standard mortality ratio (SMR) is a common measure of mortality. The dashed line represents the level of drug-related deaths among the general male population in England and Wales (SMR equals 100). When the value of the SMR per period is above 100, the risk of drug-related death is higher in the male prison population compared with peers of the same age group and sex in the population.
- Error bars show the upper and lower confidence limits, which is a margin of error around the SMR estimates. When the range of the upper and lower confidence intervals exclude 100, the risk of drug-related death for a given period is statistically different to that observed in the general male population of England and Wales.
Download this image Figure 3: The risk of drug-related deaths in the male prison population is comparable with the male general population
.png (34.1 kB) .xls (45.6 kB)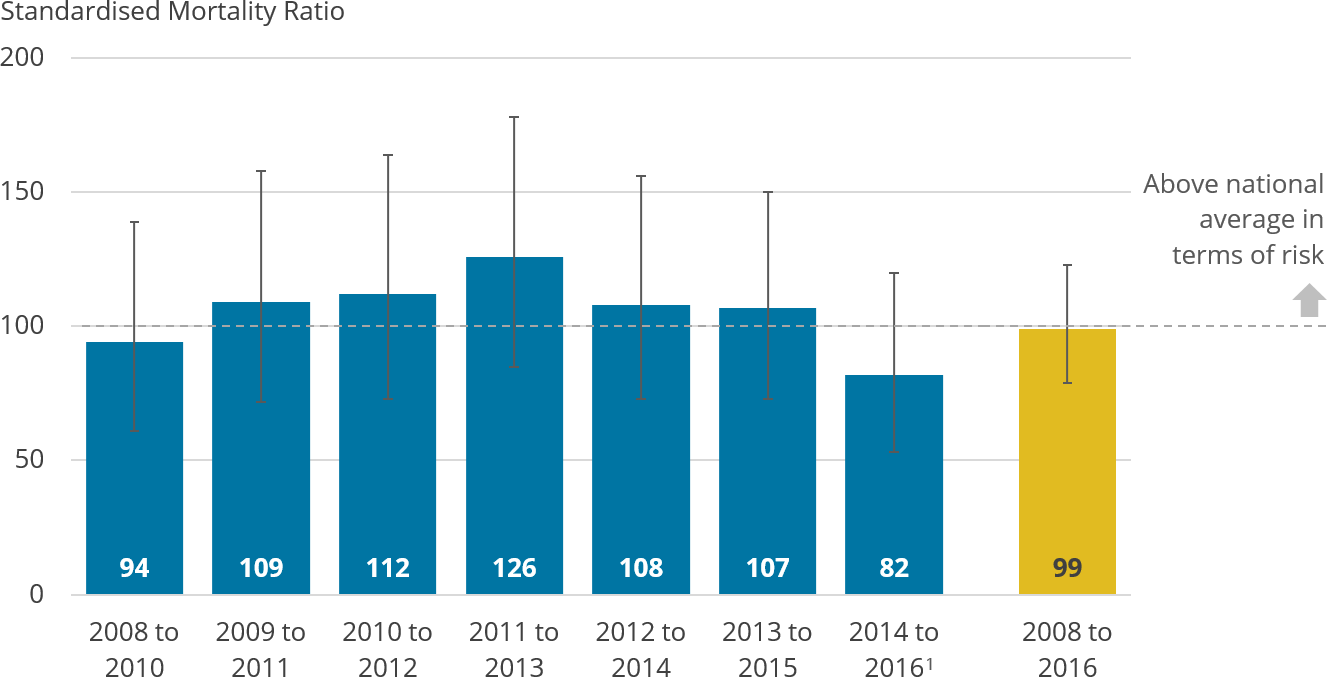{kind=link}
The rate of drug-related deaths in the male prison population has remained consistent over time despite a significant increase in the general population since 2010 to 2012 (see Figure 4). Due to the small number of deaths for this cause, changes over time will generally not be significant due to the large degree of statistical uncertainty.
Figure 4: Over time, the gap between the rate of male drug-related deaths in the prison and general population has narrowed
Age-standardised rates of male drug-related deaths, England and Wales, 2008 to 2016
Source: Office for National Statistics
Notes:
- Estimates for 2014 to 2016 are expected to be an underestimate and should be interpreted with caution.
- Figures are based on the National Statistics definition of drug-related deaths for the year the death occurred. Figures are for males aged 15 years and over.
- Age-standardised drug-related death rates per 100,000 population, standardised to the 2013 European Standard Population (ESP). Age-standardised rates are used to allow comparison between populations that may contain different proportions of males of different ages.
Download this chart Figure 4: Over time, the gap between the rate of male drug-related deaths in the prison and general population has narrowed
Image .csv .xlsDrug-related deaths by substance
Table 1 provides the number of times a specific type of substance was mentioned on the death certificate, with or without mentions of other drugs. Therefore, there are more mentions of drugs (106 mentions) than the overall number of individual deaths from drug poisoning. The figures include deaths among both males and females.
The breakdowns of selected substances provided are consistent with those reported for the general population in our annual Deaths related to drug poisoning in England and Wales statistical release.
In the period 2008 to 2016, opiates were the most common substance mentioned (62 mentions) in drug-related deaths in the prison population, with methadone (26 mentions), and heroin and morphine (25 mentions) being the most common forms. Opiates were also the most common substance mentioned in drug-related deaths in the general population during this entire period.
Benzodiazepines were the second-most common substance, with 15 mentions of the drug for drug-related deaths in prison custody; Diazepam (10 mentions) was the most common form. This was followed by eight mentions of antidepressants being involved in drug poisoning deaths in prisoners for this nine-year period. A more detailed breakdown of Table 1 can be found in our accompanying datasets.
The use and supply of drugs in prison has previously been reported on in the United Kingdom drug situation: Focal point annual report.
| Substance | Number of mentions |
|---|---|
| Any opiate (including unspecified opiates but excluding paracetamol compounds) | 62 |
| Any benzodiazepines | 15 |
| All antidepressants | 8 |
| Antipsychotics | 5 |
| Cocaine | 4 |
| New Psychoactive Substances | 4 |
| Zopiclone/Zolpidem | 3 |
| Paracetamol (includes dextropropoxyphene mentioned without paracetamol) | 2 |
| Pregabalin | 2 |
| Any amphetamine | 1 |
| Total | 106 |
Download this table Table 1: The number of drug mentions for drug-related deaths in the prison population, England and Wales, 2008 to 2016
.xls .csvComparing the cause of death recorded by HMPPS with the ONS definitions of suicide and drug-related deaths
When someone dies in prison custody, the system used by the MoJ for recording deaths in prison provides a provisional classification of the cause of death for administrative and statistical purposes. The final underlying cause of death is then determined by a coroner in an inquest. The Office for National Statistics (ONS) receives information on deaths in prison custody when a death is registered after a coroner’s inquest, which is then coded using the International Classification of Diseases.
In our linked dataset, 575 deaths were classified as self-inflicted deaths by HMPPS; the majority of these deaths (453 deaths or 79%) were included in our definition of suicide, based on the information received from the coroner (see Table 2).
Out of 575 self-inflicted deaths, 24 were classified as drug-related deaths using our definition; this figure includes eight deaths that are counted in our definition of suicide, due to the overlap in definitions.
The large majority of the remaining HMPPS self-inflicted deaths that were not classified in our definitions of suicide or drug-related deaths, were classified by the ONS as accidental hanging and strangulation (92 out of the remaining 106 deaths).
Table 2 shows that following further investigation and the coroner’s inquest conclusion, an additional nine deaths are classified in our definition of suicide that were previously classified by HMPPS as non-self-inflicted causes (for example, as a natural cause). In these cases, it would appear that the inquest conclusion has not been reflected in a revision to the provisional classification on the HMPPS database and this will be rectified in advance of future MoJ publications.
In the linked dataset, 88 deaths were classified in our definition of drug-related deaths. For drug-related deaths, the majority of these (61%) were classified by HMPPS in the group of “other”, which includes non-natural causes of death as well as deaths where further information was needed to code the cause. Of drug-related deaths, 27% were classified as self-inflicted in prison at the time of death.
Drug-related deaths are not specifically recorded by HMPPS as a cause of death, instead the death will be assigned to one of the HMPPS broad causes, depending on the evidence that was available at the time of death (for example, presence of drug paraphernalia at the scene suggesting the death was non-natural and/or a note suggesting that it was self-inflicted).
Compared with Table 2, previously published estimates in Safety in custody statistics include higher numbers for each HMPPS cause of death. Data presented here are based on the records we were able to link during the period, so include lower overall numbers.
| HMPPS cause of death | |||||
|---|---|---|---|---|---|
| ONS category | Self-inflicted | Other: Awaiting further information³ | Other: Other or non-natural³ | Natural Causes | Homicide |
| Suicide | 453 | 4 | 3 | 2 | 0 |
| Drug-related deaths | 24 | 13 | 41 | 10 | 0 |
| Other causes of death | 106 | 4 | 23 | 1135 | 24 |
| HMPPS total number of deaths¹ | 575 | 20 | 65 | 1146 | 24 |
Download this table Table 2: A comparison of the cause of death recorded by HMPPS at the time of death and how these have been categorised by the ONS
.xls .csvRegistration delays
The median registration delay for suicide deaths in the prison population in the analysis period (2008 to 2016) was 539 days compared with 151 days for the general population.
Similarly, the registration delay for drug-related deaths was 536 days in the prison population compared with 166 days in the general population during 2008 to 2016. Please see the associated dataset for the registration delay per three-year period.
The investigation of prison deaths is complex and can take additional time to establish the cause of death. Deaths in prison custody are subject to police investigation and coroner’s inquest. In the context of prison deaths caused by suicide or drugs, a jury may be involved.
Nôl i'r tabl cynnwys7. Sources of data used in this analysis
Data on deaths in prison custody held by the Ministry of Justice
When someone dies in prison custody, their death is recorded in HM Prison and Probation Service (HMPPS) Deaths in custody database. This contains summary details of each death in prison custody since 1978 and only includes those aged 15 years and above.
All deaths in prison custody are subject to a coroner’s inquest, where the coroner determines the cause of death. Before an inquest has concluded, the system used for recording deaths in prison provides a provisional classification for administrative and statistical purposes. Deaths are grouped into four broad causes of death:
natural causes: any death of a person as a result of a naturally occurring disease process
self-inflicted: any death of a person who has apparently taken his or her own life irrespective of intent; this includes all suicides and also accidental deaths as a result of a person’s own actions
homicides: any death of a person at the hands of another
other: any death of a person that cannot be easily classified as natural causes, self-inflicted or homicide; this also includes accidents and cases where the cause of death is unknown even after all investigations have concluded
In England and Wales, deaths in prison custody concern any death of a person in prison custody arising from an incident occurring during (or, on rare occasions, immediately prior) to prison custody and also includes deaths of those while released on temporary licence (ROTL) on medical grounds. Prison custody includes all public and contracted prison establishments and escort contractors.
Further information on the data source, including its quality, can be found in Guide to safety in custody statistics (PDF, 537KB).
Death registrations data held by the ONS
The Office for National Statistics (ONS) holds data on all deaths registered in England and Wales.
All suicide deaths and the majority of drug-related deaths are registered by coroners following the conclusion of an inquest. Following death registration, the ONS then assigns each death with an underlying cause based on the information provided by the coroner; with this, every death is assigned a code from the International Classification of Diseases (ICD).
For those who died in prison custody, we only have this information if the place of death was recorded as taking place in a prison itself or if this information was provided by the coroner in their inquest report.
Further information on the death registrations data held by the ONS can be found in the Quality and Methodology Information report.
National Statistics definition of deaths caused by suicide
The definition of suicide used in this article includes all deaths from intentional self-harm for persons aged 10 years and over, and deaths where the intent was undetermined for those aged 15 years and over. More details on the ICD codes used to define deaths caused by suicide can be found in the Quality and Methodology Information report.
National Statistics definition of deaths related to drug poisoning
The definition of a drug poisoning death is based on the International Classification of Diseases (ICD) code assigned as the underlying cause of death. More details on the ICD codes used to define deaths related to drug poisoning can be found in the Quality and Methodology Information report.
Drug poisoning deaths involve a broad spectrum of substances, including controlled and non-controlled drugs, prescription medicines (either prescribed to the individual or obtained by some other means), and over-the-counter medications. As well as deaths from drug abuse and dependence, figures also include accidents and suicide involving drug poisonings as well as complications of drug use (such as deep vein thrombosis or septicemia from intravenous drug use). They do not include other adverse effects of drugs (for example, anaphylactic shock), or accidents caused by an individual being under the influence of drugs. Further information can be found in our statistical bulletin on deaths related to drug poisoning in England and Wales.
It is important to note that there is an overlap between the National Statistics definitions of suicides and drug-related deaths, whereby deaths caused by intentional self-poisoning and undetermined poisoning by drugs will be included in both suicide and drug-related analyses.
Population data
Two sources of population data were used to create the statistics in this article. To define the prison custody population at risk, we used available prison custody population data (XLS, 621KB) published by the Ministry of Justice (MoJ).
Since 2010, these populations have been published on a quarterly basis, providing a snapshot of the prison population at each point in time. To produce annual populations, we took the average (mean) of the prison population across the quarters; this was not possible prior to 2010, as populations were only published for a single point each year. Despite this caveat for the earlier years (that is, 2008 to 2009), it is unlikely that this has impacted our results as the prison population only tends to minimally fluctuate on a quarterly basis.
To calculate rates in the general population of England and Wales, we used ONS mid-year population estimates to correspond to the same age bands reported in the prison service (15 to 17, 18 to 20, 21 to 24, 25 to 29, 30 to 39, 40 to 49, 50 to 59, 60 and over).
Nôl i'r tabl cynnwys8. Data linkage
In this article we identified those who had died in prison custody by linking records in our death registrations database with records held in the HM Prison and Probation Service (HMPPS) Deaths in custody database. Our research was approved by the Secretariat of the National Statistician’s Data Ethics Advisory Committee following self-assessment of ethical principles.
Overall, our analysis was only based on records we were able to link during the period between 2008 and 2016 (1,830 out of 2,040 records or 90%). Information in this section states how this was carried out.
The Office for National Statistics (ONS) was provided with a record-level extract of deaths from HMPPS Deaths in custody database for all deaths that occurred in prison custody from 2008 to 2017, inclusive. The extract contained a total of 2,338 individual records and included unique identifiers (names, date of birth), the date of death and the broad cause of death category assigned to each death (that is, natural, self-inflicted, homicide, other).
Pre-processing
Before linkage, both datasets (ONS death registrations and HMPPS deaths) underwent a basic normalisation process, to achieve consistency between both datasets. For example, all text was converted to lower case and we removed accents, punctuation and multiple spaces.
The linkage
We linked the two datasets using available unique identifiers (forename, surname, date of birth, date of death). The linkage process consisted of three join types.
Direct
We matched like-for-like records between the two datasets. We were able to match 1,503 out of 2,338 records using this technique (64%).
Approximate
For the records we were unable to match directly, we used a technique to ascertain how similar or dissimilar records between the two datasets were.
For this we used a method called Damerau-Levenshtein distance; this works by calculating the number of operations (for example, insertions, deletions, substitutions) it would take to convert one record into another. In this project, the maximum Damerau-Levenshtein distance accepted was four. Records that had a distance of two or less were accepted without review; records that had a distance of three or four were manually reviewed before being accepted. We were able to match a further 390 records using this process (17% of all 2,338 records).
Reverse
To see if any further records could be matched, from the ONS death registrations database, we extracted all deaths where the place of death was recorded as being in a prison or other similar institution (for example, remand centre, probation hostel, detention centre and so on).
Subsequently, we looked to see whether any of the returned records appeared in the HMPPS deaths data but failed to be linked via the direct or approximate methods. We were able to match a further three records using this process (less than 1% of all 2,338 records).
Results
A total of 1,896 of 2,338 records were successfully linked (81%), leaving 442 records we were unable to link (19%). Given the much larger number of non-linked records for 2017, we did not include these in our analysis. As such, our analysis is only based on records we were able to link during the period between 2008 and 2016 (1,830 out of 2,040 records provided by the MoJ during the period or 90%).
For the most recent period (2014 to 2016), due to an elevated number of non-linked records for 2016, we flag the findings for this period as preliminary and subject to change.
The vast majority of non-linked records, 364 out of 442, had a date of death in the years 2017 and 2016, as shown in Table 3. It is likely that the main reason for not being able to successfully link records for these years is because the ONS does not yet have the death registrations in the most recently available data at the time of analysis (death registrations to the end of 2017), due to incomplete coroner inquests impacting registration delays (see Section 6, registration delays).
Other reasons why we were unable to link records may include a small number of inaccuracies in HMPPS deaths data, as detailed in the Guide to safety in custody statistics (PDF, 537KB), including inaccurate date of birth, date of death and the misspelling of names.
| Date of death year | Number of non-linked records | As a proportion of non-linked records |
|---|---|---|
| 2017 | 232 | 52% |
| 2016 | 132 | 30% |
| 2015 | 33 | 7% |
| 2014 | 13 | 3% |
| 2013 | 9 | 2% |
| 2012 | 6 | 1% |
| 2011 | 5 | 1% |
| 2010 | 4 | <1% |
| 2009 | 3 | <1% |
| 2008 | 5 | 1% |
| Total non-linked cases | 442 |
Download this table Table 3: The number and proportion of non-linked records by year of death
.xls .csv9. Data analysis
Standardised mortality ratio (SMR)
Most of the findings in this article are based on the standardised mortality ratio, referred to as an SMR. This commonly used measure of mortality, for the purpose of this analysis, establishes whether the number of suicides or drug-related poisonings in the male prison population are high or low relative to patterns of risk, for these two causes, in the broader population of England and Wales (that is, all men in England and Wales aged 15 years and above). This considers the age distribution of those in prison custody.
SMRs were calculated according to the age bands used in prison services: (15 to 17, 18 to 20, 21 to 24, 25 to 29, 30 to 39, 40 to 49, 50 to 59, 60 and over). Specifically, from sex and age-specific rates of suicide or drug-related poisonings in England and Wales, we calculated how many suicides or drug-related deaths would be expected in the male prison population, should the overall pattern for these two causes of death in the male general population be the same in the male prison population. The SMR is then calculated by dividing the observed number of deaths (in the male prison population) by the expected number, expressed as a percentage:
An SMR higher than 100 indicates a greater risk among the male prison population for a given cause of death; values less than 100 suggest lower than expected risk (for example, an SMR of 150 means a 50% increase in the risk among the prison population, compared with peers of the same age group and sex in the population).
The SMR should not be used to understand how the level of risk changes over time; for this purpose, we have also included age-standardised rates. Further information on the SMR (XLS, 150KB) including how it is calculated has been published by Public Health England. Further information on age-standardised rates can be found in our Quality and Methodology Information report.
Nôl i'r tabl cynnwys10. Acknowledgements
We would like to thank Professor David Gunnell and colleagues from the Ministry of Justice for their invaluable comments on this work. We would also like to thank colleagues from our Analytical Data and Customer Service team, particularly Ben Aspey and Justine Pooley, who worked on the data linkage.
Nôl i'r tabl cynnwys